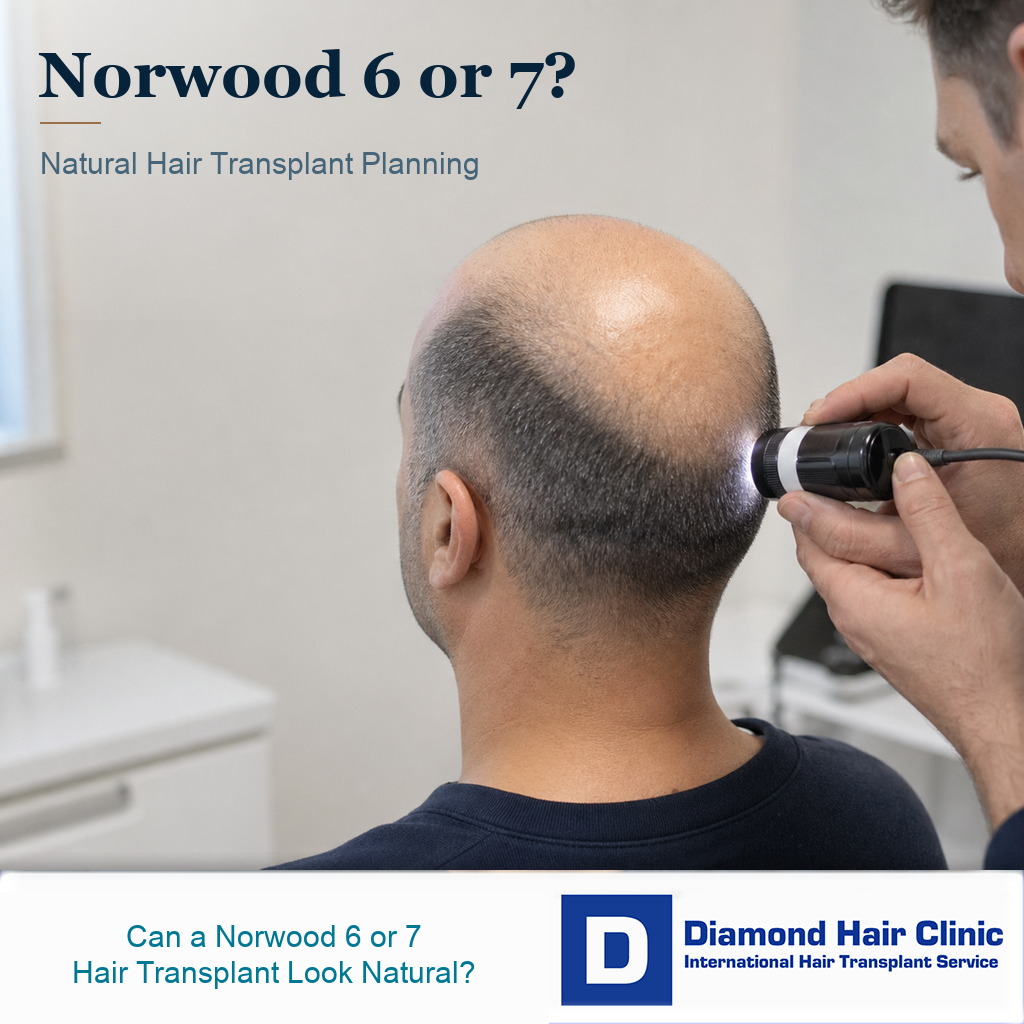
Norwood 6 or 7 Hair Transplant With Limited Donor Hair
A Norwood 6 or 7 hair transplant can look natural in patients whose case fits, but a natural result is not the same as full restoration. At this stage, the goal is usually selective coverage, with a conservative hairline, stronger framing of the face, useful middle scalp coverage, and a crown plan that accepts limits. The deciding factor is not the biggest graft number. It is whether donor supply can support the plan without being damaged. Patients who are not yet this advanced but already beyond a small hairline case can compare that middle stage in Norwood 4 or 5 hair transplant planning.
If you are already Norwood 6 or 7, the question is not only whether surgery is possible. The decision should focus on whether surgery will leave you looking more balanced while still looking natural and keeping long term donor reserve protected. That answer depends on donor capacity, hair caliber, scalp contrast, age, medical stability, crown size, beard or body hair suitability, and how clearly the plan is explained before surgery.
Patients in this stage who are considering a hair transplant in the 40s or 50s need the same balance. That means useful facial framing, realistic crown expectations, and a donor area that is not pushed past its limit.
Advanced donor strategy check
Start with the donor limit, then choose the coverage pattern
In a Norwood 6 or 7 case, I do not plan from the wish for full coverage. I separate what the scalp donor can safely do, whether extra donor sources can support the plan, which zones deserve priority, and what would make surgery too risky.
Donor check
The safe donor zone sets the ceiling
Density, miniaturization, hair caliber, previous extraction, scalp contrast, and how the donor will look with short hair.
The quote gives a large graft number before the safe zone is mapped and measured.
What number becomes safer if the donor is weaker than the photos suggest?
I must still like the donor area after extraction. Otherwise the plan is too aggressive.
Understand the limits of Norwood 6 or 7 first
Norwood 6 and Norwood 7 describe advanced male pattern baldness. In Norwood 6, the frontal area and crown have usually joined into one large bald area, with hair remaining mainly around the sides and back. In Norwood 7, the remaining donor rim is often narrower and the bald area is larger.
The practical difference is not just the label. A Norwood 6 patient with a wide, stable donor rim and coarse hair may still be a selective coverage candidate. A true Norwood 7 patient with a low, narrow, or miniaturized rim may have a much smaller surgical window, even if the desire for coverage is the same.
That difference matters because a hair transplant moves hair. It does not create new donor hair. If the bald area is very large and the donor supply is limited, the surgeon must decide where each graft will give the strongest visual effect.
The discussion must be different from a smaller hairline transplant. In advanced baldness, the plan is not only about filling empty skin. It has to create the appearance of coverage that still looks natural when the hair is dry, wet, under bright light, and viewed from different angles.
Many patients search for whether advanced baldness can be treated in one session. That is a useful question, but it is not the whole decision. A single big session may sound attractive, yet a staged or more conservative plan can be safer if the donor area needs protection.
Does donor capacity decide the plan?
The donor area sets the surgical limit. If it is strong, wide, and dense enough, the options are broader. If it is narrow, miniaturized, overharvested, or naturally weak, even an experienced surgeon must reduce the ambition of the plan.
When I evaluate a high Norwood patient, I do not begin by asking how many grafts the bald area could accept. I begin by judging what the donor area can safely give. A plan that looks impressive on paper can become a poor plan if donor supply is thinned too aggressively.
This matters most for men who want to keep the sides short. FUE extraction leaves tiny scars, and good FUE should keep them discreet, but the donor area can still look thin if too much hair is removed or if extraction is uneven. Protecting donor reserve is part of creating a natural result, not a separate cosmetic detail.
A patient with coarse hair, lower scalp contrast, and a strong donor may achieve more visual coverage than another patient with fine dark hair, pale scalp, and a narrow donor rim, even if both are called Norwood 6. The Norwood number is a starting point. It is not a surgical plan.
A Norwood 7 plan is not just a larger Norwood 6 plan. When the remaining rim is narrow, low, or miniaturized, the safe scalp donor may not support broad coverage at all. When that happens, I may discuss a very limited frontal goal, camouflage support, or not operating instead of forcing grafts into a plan that cannot look natural.
Full coverage is rarely realistic with advanced baldness
Full coverage can mean different things. If the patient means natural framing, a visible hairline, improved top coverage, and a thinner but acceptable crown, it may be realistic in the right case. If the patient means dense coverage from the frontal hairline to the crown like before hair loss, that is usually not realistic for Norwood 6 or 7.
The bald surface area is too large for most donor areas to cover at high density. When grafts are spread too widely, everything can look thin. When grafts are packed too heavily in one area, another area may be left empty. The art is deciding where density matters most and where lighter coverage will still look acceptable.
For many high Norwood patients, the front and middle scalp give the strongest change because they frame the face. The crown is larger, circular, and visually demanding. It can consume many grafts without creating the same frontal transformation.
I do not mean the crown should always be ignored. It means crown hair transplant planning has to be responsible. In some patients, crown work is delayed. In others, it is kept lighter. In a few patients with unusually strong donor capacity, broader coverage may be possible over more than one session.
The view that matters most to the patient changes the plan. A frontal frame can change how the face looks in conversation and normal photographs, while a crown view from above may still show scalp under strong light. If the patient expects the crown to look dense from above, I plan the case differently than for someone who mainly wants a natural frontal frame. That is where whether the hairline or crown needs planning first matters so much in advanced cases.
Will I need more than one surgery?
Often, yes, if the goal is more than a frontal frame. A Norwood 6 or 7 case covers a large surface area, so I usually build a stable first result instead of spending the whole donor budget in one attempt.
The first stage often prioritizes the hairline and middle scalp because these areas carry the face. Once the first result has matured, I can judge real growth, donor appearance, crown need, styling behavior, and whether a second hair transplant is worth the additional donor cost.
This does not delay the patient without reason. It avoids guessing with the entire donor reserve. If the first stage grows well and the donor still looks healthy, the second stage can be planned with better evidence. If the first stage already looks thin or the donor looks stressed, the plan may need to become more conservative rather than more aggressive.
Should the hairline or the crown be planned first?
In most Norwood 6 or 7 cases, I protect the front and middle scalp before chasing full crown density. The front is what people usually see first. A natural, age appropriate frame can make a patient look less bald even when the crown remains thinner.

The hairline must not be placed too low. A low hairline may look exciting in a drawing, but it spends grafts quickly and can look unnatural on an older or advanced baldness patient. A mature hairline is not a compromise when it is designed well. It is often the reason the result looks natural as the patient ages.
Good hairline design in a high Norwood case should look measured, not dramatic. The temples, frontal transition, density gradient, and angle of the grafts matter more than a dramatic before and after photo. If the hairline is too low or too dense for the safe donor supply, the rest of the scalp may be left with too little support.
The crown needs planning with the same discipline. A small improvement in the crown can help some patients, but a large crown promise can drain the safe donor supply. When the donor is limited, the better plan is often a natural front and a realistic crown rather than an overextended plan that looks thin everywhere.
A high graft number becomes risky when donor safety is ignored
The number becomes risky when it is offered before the donor area has been properly examined. It also becomes risky when the number is used as a sales promise instead of a surgical estimate. A patient may hear 5,000, 6,000, or 7,000 grafts and assume the larger number must be better. That is not how I judge a plan.
The same number can be reasonable in one patient and unsafe in another. The donor density, hair caliber, number of hairs per graft, scalp laxity, previous surgery, extraction pattern, and future hair loss all change the answer. A large extraction can create a thin donor and still fail to give enough coverage on top.
If a clinic talks about 5,000 grafts in one session as if it is routine for every advanced case, I ask for the examination details before accepting the number. If the promise rises toward a 7,000 graft transplant over two days, the assessment must be even more careful. Two days does not by itself make an aggressive plan safe.
The number should come after the examination, not before it. A responsible graft estimate should explain the donor limits, the area being prioritized, what will remain thinner, and what may need a second stage. If the consultation makes every part of the scalp sound equally fixable, slow down before committing.
When two surgeons give very different plans, ask both of them to draw the coverage zone and the area they would intentionally leave thin. The safer answer is not always the larger session. In advanced baldness, a surgeon who reduces the request may be protecting the donor area you still need for future loss, aging, or repair.
Beard or body hair may help selected Norwood 6 or 7 cases
Beard or body hair can help some advanced cases, but it should not be sold as a complete solution. Beard hair is usually thicker than scalp hair, so it may add visual bulk in selected areas, especially behind the frontal zone or in parts of the crown. It is not ideal for creating a soft frontal hairline.
Body hair can be more variable. Chest hair, for example, may have a different curl, growth cycle, color, and length compared with scalp hair. It may be useful as support in patients whose case fits, but it rarely behaves exactly like scalp donor hair.
When scalp donor hair is limited, beard hair for the crown can sometimes be part of the plan. The key word is part. The foundation still has to be planned around scalp donor capacity, natural hair direction, and the areas where the patient needs the strongest visual effect.
If a clinic presents beard or body hair as a way to promise full density everywhere, treat that as a warning sign, not as a shortcut. Extra donor sources can expand options, but they do not remove the need for conservative planning, proper placement, and realistic expectations.
What I write down before I accept a high Norwood plan?
For a Norwood 6 or 7 patient, the written plan should not be a single graft number. It needs to name the first priority zone, the area that will stay softer, the donor reserve I am protecting, and the reason beard or body hair is or is not being used.
There are cases where I reduce the operation after review. A narrow safe donor zone, miniaturization at the sides, old extraction marks, unrealistic crown expectations, active scalp disease, or a request for dense full coverage can change the answer from a large session to a staged plan, camouflage support, or no surgery.
I connect the high Norwood conversation to advanced baldness in one session and secondary donor source planning because improvement and restraint belong in the same discussion. The possible gain matters, but the boundary matters just as much when a donor repair problem is the price of overreach.
Which promises are risky in Norwood 6 or 7 planning?
A risky promise usually has a pattern. The clinic gives a large graft number without a serious donor examination, promises full coverage in one operation without explaining the crown or donor limits, and focuses more on the package than on the surgical trade offs.
A weak plan often sounds too easy. It may say that every area can be covered, that the donor is definitely enough, that the crown can be filled heavily, and then pressure the patient to book quickly. In advanced baldness, that kind of certainty can be more dangerous than a cautious answer.
The consultation should leave you clearer about the trade offs. You should understand why the hairline is placed at a certain height, why the crown may be lighter, why donor management matters, and why more grafts do not always mean a better result.
Before accepting surgery, ask whether you are truly a good candidate for a hair transplant at your current stage. A patient who is not a good candidate should not be pushed into surgery just because he wants hair badly. Wanting surgery and being safe for surgery are not the same thing.
How to search for a surgeon in Norwood 6 or 7
For advanced baldness, do not search only for the surgeon who promises the largest graft count. Search for the surgeon who can explain the donor rim, the hairline height, the crown tradeoff, the area that will stay thin, and the reason a second stage may be safer. If the answer is mainly “maximum grafts” or “full coverage,” get a second surgical opinion before hair transplant before booking.
Surgery can still be worth considering in the right case
Surgery is worth considering when donor supply is strong enough, the patient accepts a mature hairline, the crown expectations are controlled, and the goal is natural improvement rather than total restoration. A high Norwood patient can still feel much better with a framed face and a more balanced top, even when the density is not perfect.
I assess the patient’s styling habits. Some men are comfortable with a shorter style and light coverage. Others need enough length to create coverage with styling. Some may prefer a transplant combined with scalp micropigmentation or a hair system strategy if donor limits are severe.
The strongest high Norwood plans are clear from the beginning. They do not hide the possibility of a second stage. They do not promise a teenage hairline. They explain how the donor will be used and what area will be protected for later.
If the patient can accept those limits, surgery can still be meaningful. If the patient cannot accept visible scalp, a thinner crown, or a conservative hairline, surgery may disappoint him even if the operation is technically well done.
Waiting or not operating can be the better decision
Waiting is better when the donor area looks weak, the hair loss is still changing quickly, the patient is very young, or the expectation is full dense coverage across the whole scalp. Waiting is also better when medical treatment, scalp diagnosis, or donor evaluation has not been handled properly.
Medication can matter here, but only in the right way. If there is still miniaturized hair in the crown or middle scalp, whether medication should be tried before surgery may change timing, crown priority, or graft need. If the area is already smooth and bald, medication may still support surrounding native hair, but it will not create a new donor supply.
Not operating can be the better decision when the donor rim is too narrow or miniaturized. When that happens, surgery may move a limited number of hairs into a very large area and leave both the top and donor looking worse. That is not a conservative decision. It is a protective one.
Patients with a weak donor area need especially careful advice. Sometimes a small frontal improvement is still possible. Sometimes a non surgical route gives a cleaner and more predictable appearance. The answer should come from examination, not hope.
Telling a patient that surgery should be delayed or limited is safer than approving a plan that consumes the donor area and leaves no good repair path. Advanced baldness already makes the safe donor supply tight. A poor first plan can make the second plan much harder.