


Yellow Scalp Fluid Warning Signs
Yellow fluid after a hair transplant can be harmless healing fluid, dried serum, old bruising mixed with moisture, product residue, or infection. The color alone does not answer the question. I first want to know whether it is thin or thick, whether it smells, whether the scalp is hot or increasingly painful, whether redness is spreading, whether fever is present, and whether the area is improving or getting worse.
In the first days after FUE, a small straw colored mark on gauze or a yellow crust on part of the donor or recipient area does not by itself mean the grafts have failed. Cloudy pus, a bad smell, increasing pain, heat, fever, open skin, or one side becoming worse changes the answer. The trend matters more than the color. If the unclear sign is mainly temperature, I separate fever after a hair transplant from ordinary drainage anxiety.
Yellow fluid after FUE needs context
Yellow fluid can appear after FUE because the scalp has been treated like a surgical skin surface. Tiny channels are made, local anesthesia and fluid are used, and the skin begins to seal itself. A thin clear or pale yellow fluid can dry into a yellow crust. Old bruising can also shift color as it settles, especially around swollen tissue. The first distinction is whether you are seeing skin color, dried crust, product residue, or fresh wet fluid from one point.
That does not mean every yellow mark is harmless. A photo can make thin serum, dried product, old blood, and pus look similar. I ask whether the fluid is watery or thick, whether it is increasing, whether it is coming from one point, and whether the surrounding skin looks quieter or more inflamed than yesterday. If yellow drainage appears with swollen glands after FUE, fever, heat, or increasing pain, the urgency changes.
Amount matters as much as color. A small dry spot on gauze is different from a dressing, pillow, or neck towel that becomes wet again after you change it. If one clean blot removes the mark and it does not return, residue or old fluid is more likely. If the same point becomes wet again, or the mark is larger each time, send photos and do not wait for the next routine check.
Swelling after a hair transplant needs warning sign separation. Early swelling that moves and settles is reviewed differently from swelling that becomes hot, painful, one sided, or linked to fever and drainage.
Drainage is different from bruising
Drainage is fluid. Bruising is color in the skin or under the skin. In real recovery, they can overlap. You may see yellow staining on gauze, a pillowcase, or a cotton pad and assume infection, when the source may be thin serum mixed with old blood or the changing color of a bruise.
Bruising usually changes gradually from purple or red toward yellow or green before fading. Drainage leaves a wet or dried mark. If the yellow color is only in the skin and the area is not hotter, more painful, or spreading, I judge it differently than fluid that keeps leaking from a tender point.
The same color change logic applies when I review black eye bruising after a hair transplant. On the scalp, skin color, dried crust, and active discharge are not the same finding.
Yellow fluid signs that suggest infection
Yellow fluid becomes more concerning when it is thick, cloudy, greenish yellow, smelly, or increasing instead of settling. I also pay attention to spreading redness, warmth, tenderness, swelling, fever, chills, worsening pain, and a point that opens or keeps draining. When odor is the first clue, scalp odor during FUE recovery explains how smell, fluid, warmth, and fever fit together.
Thin pale yellow fluid behaves differently from thick opaque pus. Pus often looks cloudy, creamy, yellow white, yellow green, or brown, and it may smell unpleasant. If the fluid is thick or the skin around it is painful and hot, treat that as a review issue even if the total amount looks small.
A worry about graft survival can make patients miss the more important concern, which is whether the skin is becoming infected. Mild crusting can belong to early healing, but pustules, spreading redness, and painful bumps need a different level of attention. When those signs appear, I separate them the same way I separate redness, scabs, and pimples after a hair transplant. A wider infected hair transplant pattern is judged by trend, pain, heat, discharge, fever, and whether the scalp is moving in the wrong direction.
If the picture looks like inflamed follicles or pus around hair shafts, I also think about folliculitis after a hair transplant. Folliculitis is not judged by color alone. Pain, pustules, recurrence, and spreading inflammation matter.
Color alone is not enough. The texture, smell, pain, heat, fever, and trend decide how urgently the area needs review.
Use the 10 yellow fluid slides below to judge texture, smell, pain, heat, fever, trend, and when a photo or local review matters. Swipe the carousel, use the arrows for one step at a time, or choose a number below the image to jump to that point.



Check before touching or washing the area
Before touching the area, stop and look. First ask where the fluid is. It may be on the donor area, recipient area, forehead, behind the ear, or pillow. Is it watery, sticky, thick, cloudy, or crusted? Is there a smell? Is the surrounding skin hotter or redder than the other side? Is pain increasing? A photo before any wiping is more useful than a photo after repeated cleaning attempts.
Do not squeeze, scrape, or dig at the yellow area. Squeezing can irritate tissue, open crusts, introduce bacteria, or make a small problem look larger. If the clinic has given washing instructions, follow those instructions gently instead of inventing a stronger cleaning method because the color worries you.
Do not scrub the scalp with alcohol, hydrogen peroxide, harsh antiseptic, perfume, or repeated disinfectant wipes unless your clinic specifically told you to use that product. Strong cleaning can irritate healing skin, disturb crusts, and make the surface look worse before anyone can judge the real problem.
Gentle washing after a hair transplant matters here because early cleaning is controlled. The point is to soften and clean the area without rubbing grafts or breaking fragile healing skin.
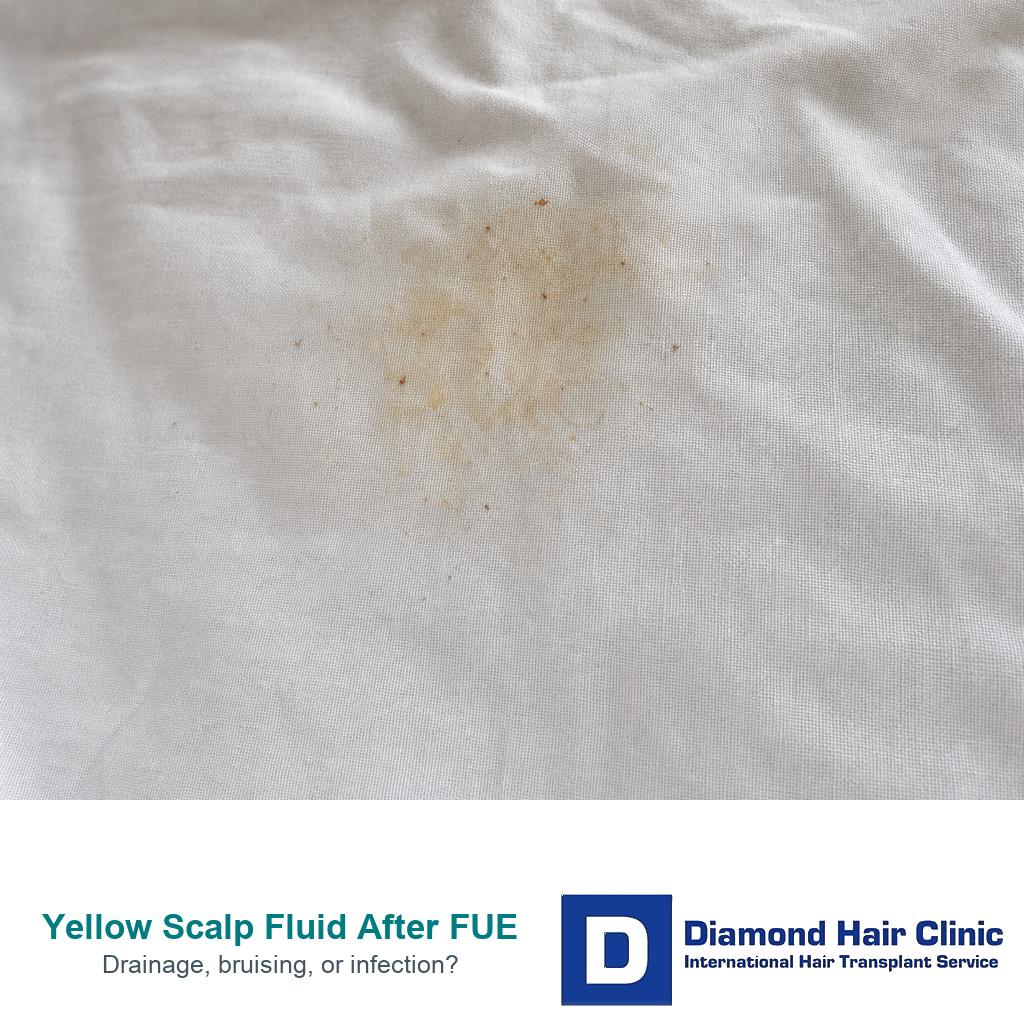
Yellow pillow stains come from the donor area
Yellow stains on a pillow or neck pillow can come from the donor area, especially in the first few days. The donor area is often in contact with the pillow, gauze, or headrest. A small amount of pale yellow or pink yellow fluid may dry on fabric and look more dramatic than it is. Change to a clean pillowcase before judging recurrence, because yesterday’s dried mark can make today’s scalp look worse than it is.
A stain needs context. One small mark is different from a repeated wet leak. A small dried stain on skin that is settling is different from ongoing fluid, increasing pain, swelling, bad smell, or fever. Also check whether the mark is actually from ointment, shampoo residue, saline, sweat, or old blood diluted by moisture.
If there is blood, mixed fluid, or panic about sleeping pressure, compare the finding with blood on the pillow after a hair transplant because graft contact, donor seepage, and sleep related checking need their own review.
Yellow fluid does not always damage grafts
Yellow fluid itself does not pull grafts out. Grafts are more directly threatened by trauma, scratching, rubbing, strong pressure, infection, heavy bleeding, or aggressive cleaning. A thin dried mark is not the same as a lost graft.
The risk becomes more serious if the yellow fluid represents infection, if you scrape crusts away, or if repeated checking causes rubbing. It is possible to irritate the area while trying to prove that nothing is wrong. One clear photo, a factual message, and hands away from the grafts give a better answer.
If you see tissue, a hair with surrounding tissue, or a gap after crust removal, the distinction in scabs and lost grafts after a hair transplant becomes useful. A yellow crust and a lost graft are different questions, but anxiety can make them feel identical in the first week.
Do not change antibiotics or creams on your own?
Do not start, stop, double, or replace antibiotics because of a yellow photo alone. If antibiotics were prescribed, I need to know the exact medicine, dose, timing, missed doses, allergies, stomach symptoms, and what the scalp looks like today compared with yesterday.
Topical creams or ointments are similar. Too much product can leave yellow residue or trap moisture. Too little treatment can leave irritation uncontrolled if the clinic specifically prescribed something. The answer depends on the original operation, the area involved, and the current symptoms.
Antibiotic decisions after surgery need the same precision described in antibiotics after a hair transplant. They should not be copied from another patient online. Medication changes need your own clinic context.
A useful message shows the source, timing, symptoms, medicines, washing routine, and whether the yellow area is spreading or settling.
Photos and details to send
Send one clear close photo, one wider photo showing the location, and a short timeline. Say the day after surgery, when the yellow fluid started, whether it is donor or recipient area, whether it is increasing, whether there is pain, heat, redness, swelling, smell, fever, or chills, and what products or medicines have touched the area. Also mention diabetes, immune problems, steroid medication, smoking, or any other healing risk your local doctor already follows.
Describe the amount in plain language. It may be one small dry mark, a coin sized wet spot, repeated drops, a soaked gauze, or fluid that returns after wiping. If washing is already allowed, a photo before gentle washing and another after the area is dry can help separate residue from active drainage.
A message that says “is this infection?” is less useful than a message that says “day four, donor area, watery yellow mark on pillow, no fever, no smell, mild tenderness, same size as yesterday, washed once with the clinic shampoo.” A remote clinic can make a better decision when the pattern is visible.
Hair transplant follow up after surgery works best when the clinic receives source, timing, symptoms, medicines, and photos together. A timeline matters more than only a close photo.
Signs that separate yellow fluid from bleeding scabs and necrosis
Bleeding is red or dark red active blood. Yellow fluid is different, although old blood and serum can mix and change the color. If the concern is active bleeding, pressure, trauma, or a visible lost graft, compare the situation with bleeding after transplant.
Scabs are dried material on the surface. They can be brown, yellow, or mixed in color. A crust that is dry and gradually softening during washing is not the same as thick discharge that keeps coming from a painful point. Do not scrape scabs because the color looks unpleasant.
Necrosis is a much more serious tissue problem and should not be reduced to “yellow crust.” Severe pain, dark or black tissue, poor skin appearance, spreading tissue damage, and delayed healing need urgent review. If that is the concern, use the warning signs in hair transplant necrosis and ask for clinic review or seek local medical assessment quickly.
Local medical review should not wait
Do not wait for a routine message reply if yellow drainage comes with fever, chills, hot spreading redness, worsening pain, rapidly increasing swelling, confusion, faintness, a bad smell, thick pus, or an open area that is getting worse. These are not only cosmetic concerns. They are infection and wound warning signs, and surgical wound infections commonly declare themselves within the first month after surgery.
This matters especially when you are recovering abroad. Time zones, weekends, travel plans, and language barriers can delay the response. If the symptom pattern is severe, local medical review near the hotel or at home may be needed while the transplant clinic is also informed.
If you need local medical review, bring the surgery date, clinic instructions, medicines taken, allergies, and recent photos. Do not let the assessment become only a cosmetic discussion. The clinician needs to judge whether there is a skin infection, wound opening, or spreading inflammation.
There is no benefit in pretending every yellow mark is harmless, and there is no benefit in panicking over every dried stain. The decision should be practical. Ask whether the area is stable and improving, or whether it is painful, hot, wet, smelly, spreading, or linked to fever.
My judgment on yellow scalp fluid after FUE
I judge yellow scalp fluid after FUE by separating three questions. First, is it skin color, dried crust, or active fluid? Second, is the trend improving, stable, or worsening? Third, are there warning signs such as heat, spreading redness, pain, smell, cloudy pus, fever, or an open area?
If the area is settled, the fluid is thin, the amount is small, and the trend is improving, the next step is usually gentle washing according to instructions, photo monitoring, and a clear message to the clinic if uncertainty remains. If the area is worsening or has infection signs, the next step is review, not more online comparison.
Safety comes before graft anxiety. The best response to yellow fluid is not denial and not fear. It is careful observation, no scraping, a useful photo message, and fast review when the symptom pattern is no longer settling.