


- Written by Dr.Mehmet Demircioglu
- Estimated Reading Time 10 Minutes
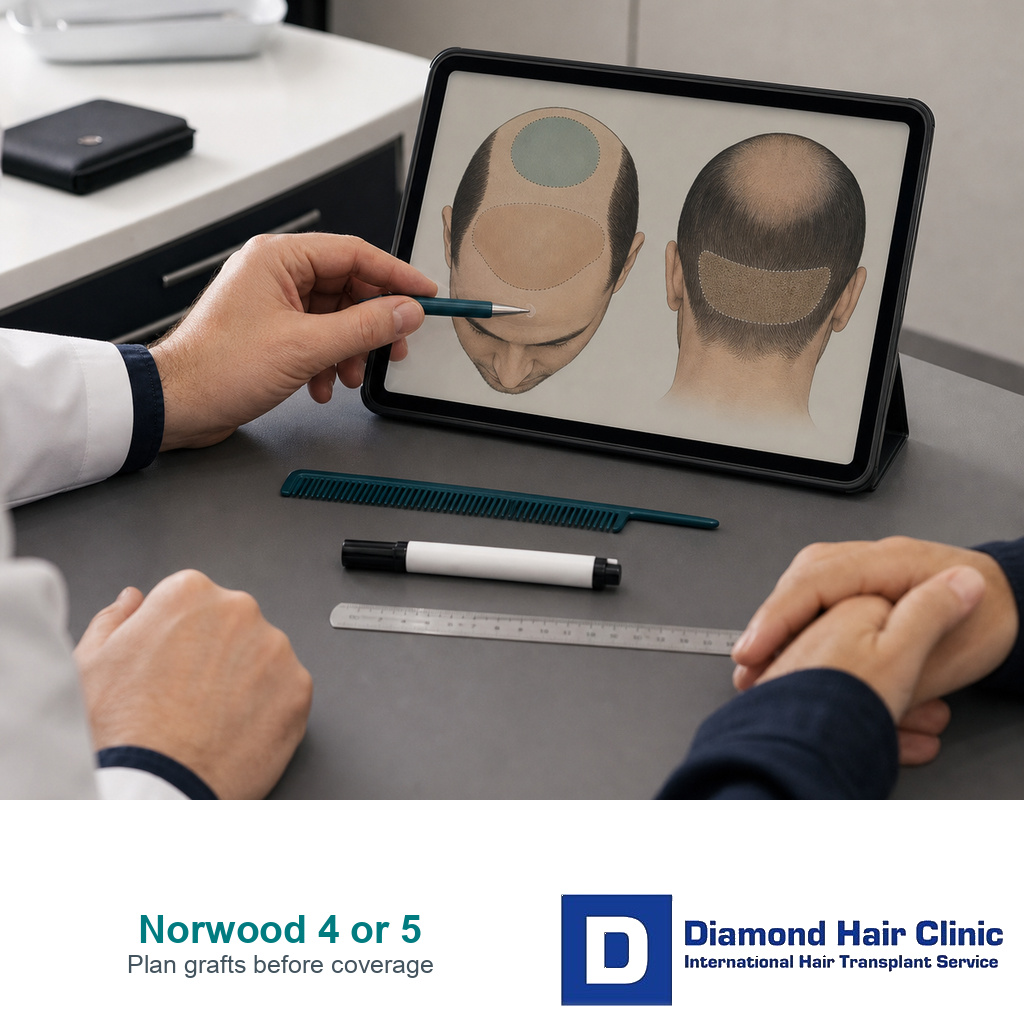
Norwood 4 or 5 Hair Transplant Planning Needs a Graft Budget
At this stage, I do not begin by asking how many grafts can be packed into one operation. I first decide what those grafts must protect for the rest of the patient’s life. Norwood 4 or Norwood 5 hair loss is already beyond a small hairline change, but it is a different problem from an advanced Norwood 6 or 7 case. The plan has to spend a limited donor supply with discipline.
The hard part is that every attractive promise uses the same graft bank. A lower hairline uses grafts. A dense front uses grafts. A bridge through the midscalp uses grafts. Crown coverage uses many grafts and often gives a softer visual return. If future hair loss continues, the patient still needs reserve. For me, the graft budget matters more than the biggest advertised number.
The first decision is not the graft number
A patient may arrive with three clinic estimates. One says 3,500 grafts, one says 4,500 grafts, and one says 5,500 grafts. That range looks like a technical disagreement, but often it is really a design disagreement. One clinic is spending more on a low, dense hairline. Another is trying to reach the crown. Another is spreading grafts thin across a large area. The number alone does not tell you whether the plan is wise.
A better first question is where the grafts are going. How much is reserved for the frontal frame? How much is needed to connect the midscalp so the top does not look divided? Is the crown being treated now, reduced, or saved for later? What donor area remains if native hair continues to miniaturize? These questions are more useful than chasing the highest graft quote.
The broader lifetime graft planning conversation matters here. A hair transplant is not a single day purchase. It is the planned use of a limited donor resource over many years. A Norwood 4 or 5 patient needs that idea before the first recipient site is made.
Norwood 4 and Norwood 5 are not the same surgical problem
Norwood 4 usually means the frontal recession and top thinning have become more established, often with crown involvement beginning or already visible. Norwood 5 means the balding bridge between the front and crown is weaker, and the total area needing coverage is larger. Two patients may both say they are “around Norwood 5,” but one still has useful midscalp hair and another has almost no bridge left.
The difference changes planning. If the midscalp bridge is still present, the operation may be able to reinforce the front and protect the visual connection to the crown. If the bridge is weak, the plan has to decide whether to rebuild that connection or accept a more staged approach. If the crown is large and expanding, chasing it too early can dilute the front and still leave the back looking thin.
For earlier recession, Norwood 3 hair transplant planning shows why restraint still matters. For advanced loss, Norwood 6 or 7 hair transplant planning shows why limits become stronger. Norwood 4 or 5 sits between those two situations, which is why the decision is often misunderstood.
A low hairline can steal from the crown later
Many patients judge a plan by the proposed hairline. I understand why. The frontal frame is what you see in the mirror, in photos, and in conversation. But at Norwood 4 or 5, a low adolescent hairline can take grafts away from the midscalp and crown before we know how the rest of the pattern will behave.
A natural hairline should match age, face shape, donor supply, hair caliber, and likely future loss. Recreating a teenage front edge can make the top look patchy later. A slightly more mature hairline with stronger density behind it can look more natural and age better than a low line that consumes too much donor capacity.
This is where hairline or crown first becomes a real planning question. The front usually gives the strongest visual change, but that does not justify ignoring the crown completely. It means the crown decision has to fit the donor math instead of competing with it blindly.
Crown coverage needs a sober conversation
The crown is a wide spiral area. It can swallow grafts quickly because the hair changes direction and the surface area may be larger than it appears in a single photo. Patients often ask for the crown to be “filled in” at the same time as the front, but a crown can demand more grafts than the result will visually repay.
That does not mean the crown should never be transplanted at Norwood 4 or 5. It means I need to know the size of the crown, the strength of the donor area, the patient’s age, medication history, hair caliber, styling goal, and whether the frontal half can still be made stable. A small crown may be reasonable. A large, expanding crown may need a delayed or limited plan.
The dedicated crown hair transplant article explains why this area behaves differently from the hairline. For Norwood 4 or 5, the crown is often the difference between a strong lifetime plan and an overextended first surgery.
Use the four slide graft budget review below to see where a Norwood 4 or 5 plan usually spends, saves, or stages grafts.

The slides are not a graft calculator. They show the tradeoff. If more grafts are spent in one zone, fewer are available for the other zones or for future loss. Every zone competes with the same donor bank.
Use this graft budget map before accepting a plan
This proof check component is for patients comparing clinic recommendations. Select the zone that sounds most important to you, then read what it usually costs in the overall plan.
Hairline frame
The front creates the strongest social change, but a low hairline can consume grafts that the top and crown may need later. Ask whether the proposed height still leaves reserve.
Midscalp bridge
The bridge stops the result from looking like a front transplant with a separate bald crown. If it is weak, the plan may need to prioritize connection before crown ambition.
Crown demand
The crown can use many grafts because the area is broad and the whirl changes direction. Treat it as a staged decision when donor supply or future loss is uncertain.
Future reserve
Reserve is not wasted graft supply. It is protection against progression, donor miniaturization, repair needs, and the possibility that one session cannot do everything safely.
Medication history changes the plan
Medication does not create donor hair, but it can change the planning confidence. If a patient has been stable on finasteride, dutasteride, minoxidil, or another medical plan under proper guidance, I may have more confidence about how fast the native hair is changing. If the patient is young, losing hair quickly, and has never tried medical stabilization, a very aggressive transplant plan becomes more risky.
This is not a blanket rule that every patient must take medication before surgery. Some patients cannot use certain medicines, do not tolerate them, or choose not to. The point is that the surgical plan should not pretend future loss is frozen when it is not. A Norwood 4 or 5 patient with active progression may need a higher hairline, lower density target, staged crown plan, or a more conservative first surgery.
If the donor itself shows miniaturization, the caution becomes stronger. The donor miniaturization and safe zone discussion is important here because transplanted hair is only as reliable as the donor area we choose to use.
The donor area decides how brave the plan can be
Two patients with the same Norwood number can have very different donor capacity. Hair caliber, density, color contrast, scalp laxity, curl, safe zone strength, prior extractions, and donor miniaturization all change what can be done. A patient with thick hair and strong donor density can sometimes tolerate a broader plan. A patient with fine hair and weak donor density may need a narrower design even if the balding pattern looks similar.
A front view alone is not enough for Norwood 4 or 5 surgery planning. The donor area must be examined carefully. It is also important to decide how much can be harvested without creating visible thinning, patchiness, or overharvesting. A plan that looks impressive on the recipient side can still be a bad plan if the donor has been sacrificed.
The donor area and weak donor area articles explain why donor quality is not a small detail. At this stage, donor protection is not conservative language. It is the foundation of the result.
A one session promise needs a second look
Some Norwood 4 or 5 patients can have a strong first surgery. Still, full front, midscalp, and crown restoration in one operation is not a responsible promise for every patient. When the recipient area is large, density must be distributed with restraint. If the clinic promises complete coverage with a very high graft number, ask where those grafts are coming from and what donor evidence supports the claim.
Large sessions can be useful in selected patients, but they can also become a way to hide poor planning behind a big number. A 5,000 graft conversation should include donor safety, surgical time, graft handling, density distribution, and what remains for the future. It should not be only a sales sentence.
The 5,000 graft FUE hair transplant discussion is useful because it separates a large session from a better operation. For Norwood 4 or 5, the question is not only whether the number is possible. The question is whether it is the right use of the donor bank.
Photos alone can miss the real risk
Remote photos can show the general pattern, but they can also mislead. Wet hair, flash, styling, crown angle, and lens distance can make the same scalp look very different. Photos also do not show donor miniaturization reliably, scalp characteristics, hair shaft diameter, or how the hair behaves under direct examination.
Photo planning can be a useful first filter. It can help decide whether a case deserves a consultation, which areas look most important, and whether the request is realistic. But a final Norwood 4 or 5 plan still needs donor examination and long range judgment.
This is where planning a hair transplant from photos has limits. A clinic can estimate, but the responsible plan must stay flexible until the surgeon can confirm the donor and recipient conditions.
My planning approach for a Norwood 4 or 5 patient
I start by defining the pattern, not just naming it. Is the patient closer to Norwood 4 with a useful bridge, or closer to Norwood 5 with a larger bald zone? Is the crown small, large, expanding, or stable? Is the front still worth rebuilding strongly, or would a lower hairline create a donor problem later? These are clinical questions, not cosmetic preferences alone.
Then I separate the plan into zones. The frontal hairline and forelock need a natural frame. The midscalp needs enough connection that the result does not look split. The crown must be judged by size, expectation, and donor cost. Finally, some grafts must remain outside the first surgery in case native hair continues to thin.
When the donor is strong and the pattern is stable, the plan can be more ambitious. When the donor is weak, the patient is young, the crown is large, or the hair loss is active, the plan should become more selective. A good Norwood 4 or 5 plan leaves a future plan possible. That is the difference between spending grafts and investing them.
The plan should make the tradeoff visible
Before accepting surgery, ask the clinic to explain the tradeoff in plain language. Which area is being prioritized? Which area is being delayed or kept softer? What happens if the crown expands? What donor reserve remains after the proposed extraction? If you cannot get a clear answer, the graft number is not enough.
A strong plan does not need to promise perfect coverage everywhere. It should show why the chosen hairline height, density, crown approach, and donor harvest fit your long range pattern. At Norwood 4 or 5, the responsible answer may be a strong front now, a conservative crown, and a second stage option later. For some patients, that is a better result than trying to solve every area at once.
My advice is simple. Do not judge the plan by the biggest graft number or the lowest hairline drawing. Judge it by whether the donor supply, hairline design, midscalp bridge, crown demand, and future loss are all being respected at the same time. That is how a Norwood 4 or 5 transplant has a better chance of looking natural now and still making sense years later.