Tinea Capitis Must Settle Before FUE Planning
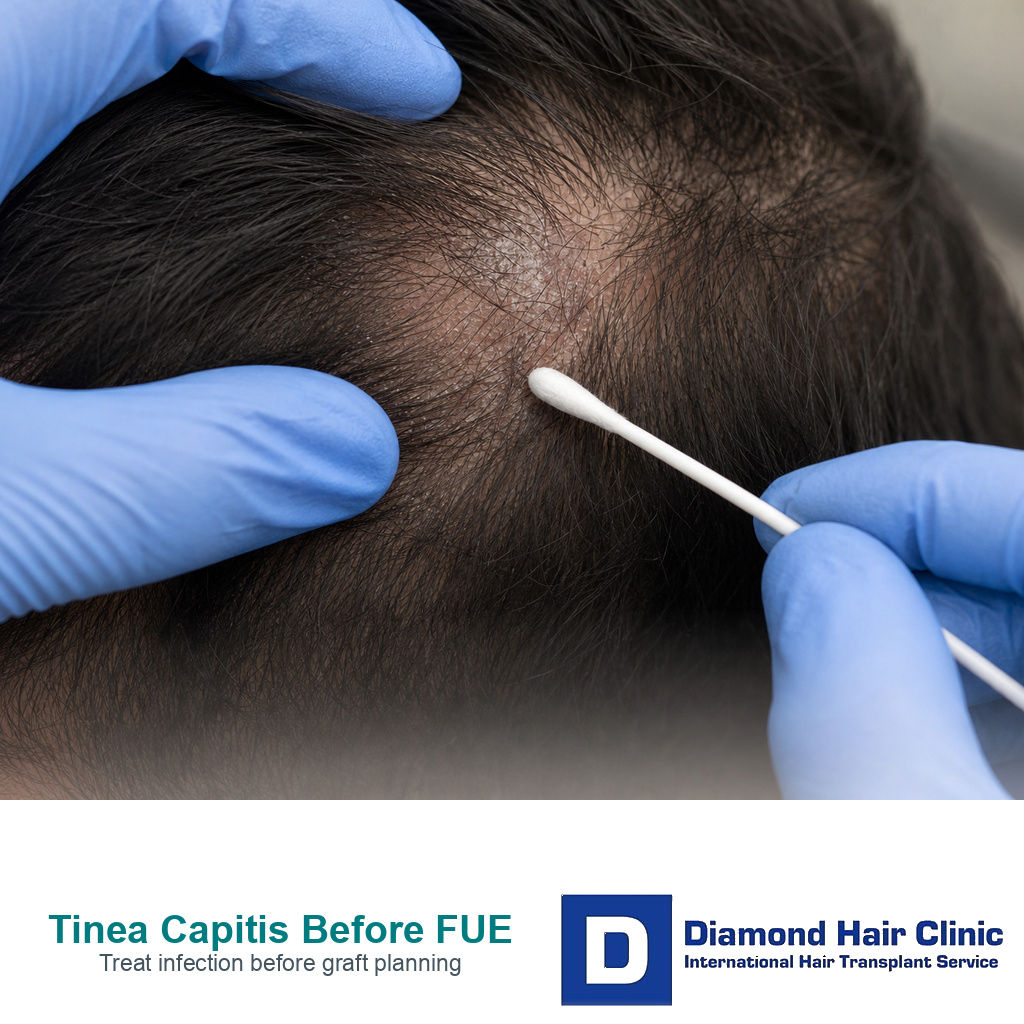
Tinea capitis can leave a bald patch that looks like a hair transplant problem, but I treat active scalp ringworm as an infection first. If the scalp is scaling, itchy, swollen, tender, crusted, draining, or showing broken hairs, I do not treat the area as ordinary stable hair loss. Before any graft plan, I need to know the diagnosis, the treatment used, and whether the scalp has truly settled.
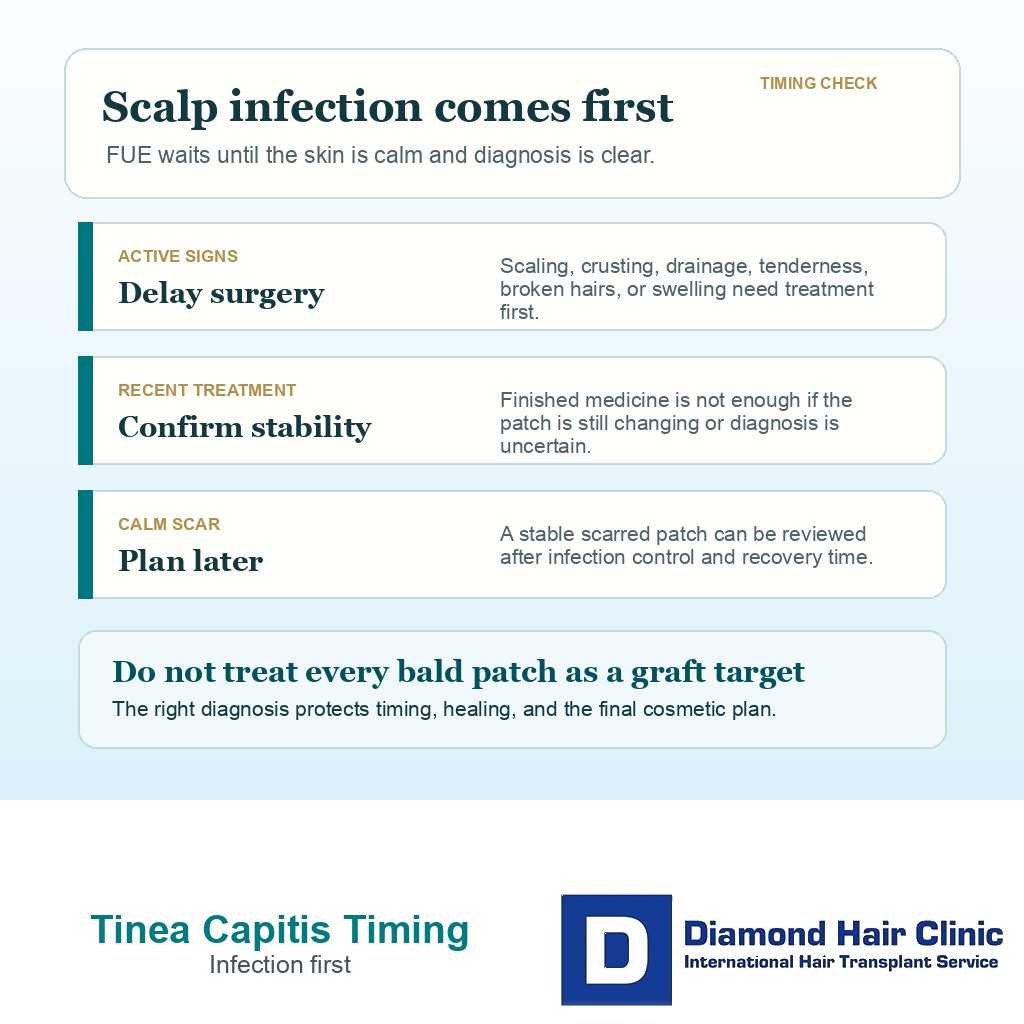
You may be able to discuss FUE later, especially if tinea capitis has left a permanent scarred patch. But surgery should not be planned while the infection is active, recently uncertain, or still changing. Active scalp infection is a reason to delay FUE, not a reason to rush grafts into the patch. A finished prescription answers only one part of the decision. I still want to know whether the infection has cleared, whether hair has had time to return, and whether any remaining patch is scarred and stable enough to graft.
Tinea capitis changes transplant timing
Tinea capitis is scalp ringworm, a fungal infection involving the scalp and hair shafts. Despite the name, it is not caused by a worm. It can produce scaling, itching, broken hairs, black dot areas, patchy shedding, or a swollen inflammatory lesion called a kerion. Some cases look mild in photographs. Others create enough inflammation to damage follicles and leave a permanent bald patch.
Hair transplant surgery works by moving follicles into skin that can receive, hold, and heal around grafts. An infected or inflamed scalp is not that setting. Grafts need clean handling, stable tissue, and predictable healing. If the diagnosis is unclear, I cannot know whether the visible patch is temporary shedding, inflammatory damage, scarring, alopecia areata, or another scalp disorder.
I do not reduce this decision to a simple gap filling exercise. What matters is whether the scalp is medically ready for surgery and whether grafting would actually solve the cosmetic problem. General hair transplant candidacy also depends on diagnosis, donor planning, scalp stability, and realistic expectations.
Active scalp ringworm means waiting
Active scalp ringworm is contagious and still needs medical treatment. It can spread through close contact, shared brushes, hats, bedding, barber tools, pillows, or sometimes a household pet. Surgery adds recipient incisions, washing, dressings, and healing demands to a scalp that first needs infection control.
For graft placement, the skin that would receive grafts needs to be settled, clean, and not inflamed. Active scale, crust, swelling, tenderness, drainage, broken hairs at the edge of the patch, or persistent itch means the tissue is not ready. Transplanting into that environment can complicate healing and make the result harder to interpret later.
The same surgical principle appears in folliculitis hair transplant planning because active infection or inflammation needs assessment before surgery. Tinea capitis is a different diagnosis, but the order is the same. Infection control comes before cosmetic graft placement.
Scalp warning signs pause the plan
I pause when the scalp shows circular or irregular scaling, broken hairs, black dots, redness at the edge of a patch, persistent itching, swollen tender plaques, crusting, drainage, lymph node swelling, or a recent diagnosis of scalp ringworm. I also pause when steroid creams were used on an undiagnosed rash, because steroids can change how ringworm looks and may allow it to spread.
Photos help, but they often miss the clues that separate fungal infection from other scalp conditions. A flaky patch may be seborrheic dermatitis, scalp eczema, scalp psoriasis, tinea capitis, traction injury, alopecia areata, or scarring alopecia. The wrong label can push you toward the wrong treatment or the wrong surgery date.
If the main symptom is itching before surgery, I still ask what sits behind the itch. In that setting, scalp itching before hair transplant surgery is a timing question, not only a comfort issue. Tinea capitis is different from many flaky scalp conditions because scalp ringworm usually needs prescription oral treatment.
Diagnosis comes before graft numbers
Diagnosis protects you from treating every bald patch as a transplant target. A small round patch may be fungal infection, alopecia areata, scarring alopecia, traction, or a healed injury. Those conditions do not behave the same way after surgery.
For suspected tinea capitis, dermatology evaluation may include scalp examination, dermoscopy or trichoscopy, hair sampling, scraping, fungal culture, or other tests. If the appearance is atypical or scarring disease is possible, a scalp biopsy before hair transplant may be part of the wider diagnostic discussion. This is not a delay for its own sake. It prevents a graft plan from being built on the wrong disease.
A transplant plan built on the wrong diagnosis can fail even when the surgical technique is careful. Surgery moves hair. It does not treat active fungal infection, stop inflammatory scalp disease, or reverse scar tissue that has already replaced follicles.
Hair may return after treatment
Hair can grow back after tinea capitis treatment when follicles are still alive and inflammation has not caused permanent scarring. It is common to worry when a patch looks bare during treatment, but the first step remains infection clearance. A transplant decision made too early can spend grafts on an area that might recover by itself.
The recovery timeline depends on the severity of inflammation, how long the infection was present, whether treatment was adequate, whether the infection returned, and whether a kerion or scarring process developed. I avoid promising regrowth from photos alone because a smooth scarred patch and a recovering patch without scarring can look similar in casual lighting.
After treatment, I want to see whether scaling, itch, crust, tenderness, drainage, and edge activity have stopped. Then I look at hair return, patch texture, skin shine, follicular openings, and the stability of surrounding hair. The right surgical timing comes after the medical behavior of the patch is clear.
Scarred patches are a later surgical question
A healed scarred patch after inflammatory tinea capitis is different from active scalp ringworm. Active infection needs medical treatment. A stable scar is a later surgical question. Scar tissue may have less flexible skin, altered blood supply, and less predictable graft survival. The area also needs to be free from active infection and medically stable.
The closest surgical comparison is hair transplant into scar tissue. The plan may need cautious density, fewer grafts per square centimeter, staged placement, and realistic expectations about coverage. In some cases, a small first session or test area is more responsible than trying to fill the whole patch at once.
I also keep scarring alopecia and lichen planopilaris in mind when a patch looks scarred or inflamed. A history of fungal infection does not exclude another inflammatory diagnosis. If the scalp is still active, the surgical answer waits.
Similar scalp conditions need different plans
Tinea capitis is an infection. Seborrheic dermatitis is usually a chronic inflammatory scalp condition often linked with yeast. Eczema involves the skin barrier and inflammation. Psoriasis is immune driven inflammation. Alopecia areata is an autoimmune hair loss pattern. Scarring alopecia damages follicles through inflammatory destruction. They can overlap in appearance, especially in photographs.
The difference matters because treatment, contagiousness, and surgical timing are different. With seborrheic dermatitis, the question may be scalp control before surgery. With tinea capitis, the infection must be treated and cleared first. With active scarring alopecia, disease control may need to be stable for a long period before grafting is considered.
A flaky bald patch is not a cosmetic blank space. I treat it as a diagnosis question first. The diagnosis has to be clear before I decide whether FUE belongs in the plan.
Treatment details must be clear before surgery
Scalp ringworm usually needs prescription oral antifungal treatment because the fungus involves the hair shaft and follicle area. Antifungal shampoo may reduce spread, but shampoo alone is usually not enough for scalp ringworm. A bottle of shampoo at home is different from a completed treatment plan from the treating physician or dermatologist.
For hair transplant planning, I need to understand the medical treatment course before surgery is scheduled. The consultation should include the diagnosis, medication name, dose if known, treatment dates, response, any liver or blood test monitoring requested by the doctor, and any other medicines that affect healing or infection risk. I do not want a patient stopping, restarting, or changing antifungal medicine around surgery without the treating doctor’s guidance.
If you have drug allergies, recent secondary infection, or a complex medication history, disclose it before surgery. An antibiotic allergy before FUE is a separate topic, but the same disclosure habit matters here because the clinic should know what was prescribed, what was tolerated, and what still needs follow up.
Use the 8 tinea capitis planning slides below to separate active infection, diagnosis, treatment details, warning signs, hair return, scar stability, cautious density, and consultation records. Swipe the carousel, use the arrows one step at a time, or choose a number below the image to jump to that point.