



Fresh donor areas need time before active topicals
The early donor area does not need a crowded routine. It needs the clinic’s washing instructions, the right timing, and no unnecessary products. A metformin cream may also contain preservatives, penetration enhancers, alcohol bases, fragrances, or other ingredients that are not obvious from the product name.
Open extraction sites are different from closed, quiet donor skin. A product that seems mild on intact skin can sting, inflame, clog, or contaminate a fresh wound field. It can also make the donor harder to read. Redness, tenderness, bumps, heat, crusting, or fluid may be irritation, but they can also be early infection or folliculitis.
Bumps and inflamed follicles need diagnosis, not experimentation, especially when folliculitis after hair transplant is possible. Spreading redness, worsening pain, pus, fever, open wounds, increasing swelling, or a generally unwell feeling should lead to clinic review or local medical assessment, not another topical layer.
Fresh donor skin needs a clear medical reason before any experimental topical product is added.
Why do compounded metformin creams need review?
Metformin tablets are common, but that does not make every topical preparation predictable. A study lotion, a cream made by a pharmacy, and a crushed tablet in a home mixture are not the same product. A prescription tablet should not be turned into a donor area cream at home. Even two compounded creams can differ in concentration, base, stability, penetration, sterility, storage, expiry, and instructions.
Oral metformin is a separate medical issue. If you take it for diabetes, PCOS, insulin resistance, or another reason, do not stop it, reduce it, or turn it into a topical experiment because of donor regeneration claims online. The prescribing doctor should guide that decision. For surgery, it should be part of the full medication before hair transplant review so anesthesia, wound healing, diabetes control, and timing are understood.
I am not against future topical research. I am against casual use of unverified mixtures on surgical skin. A fresh FUE donor area is not the place to test a homemade compound.
What do I review before allowing a topical product?
I start with timing. Is the donor skin still open? Are scabs present? Is there itching, burning, wet crusting, discharge, pain, or spreading redness? Has another product already been used? Could the product touch the recipient area as well? These details decide whether the answer is no, wait, stop, or come for review.
Then I review the product itself. I need the exact ingredients, concentration, base, pharmacy source, prescriber, storage instructions, application area, frequency, and reason for use. I also ask about diabetes, kidney disease, allergy history, eczema, psoriasis, seborrheic dermatitis, acne medication, previous poor wound healing, and whether postoperative instructions have been difficult to follow.
The goal matters too. If the goal is itching relief, there may be a simpler option approved by the clinic. If the goal is scar reduction, skin closure and timing matter. If the goal is donor regrowth, I explain that this is not proven. I judge antibiotic ointment after hair transplant by timing and indication too. A topical product can sound protective, but the wrong timing or wrong indication can create a new problem.
How should verteporfin and regeneration claims be judged?
Many people find topical metformin while reading about verteporfin and donor regeneration claims or scarless wound healing. The attraction is clear. If donor scars could be reduced and follicles could regenerate, the limits of hair transplantation would change dramatically.
That is exactly why the proof standard must be high. A donor regeneration claim affects graft numbers, hairline design, crown planning, repair options, donor reserve, and long term expectations. It cannot rest on early studies, isolated experiments, clinic marketing, or enthusiasm.
Experimental peptide products after hair transplant, copper peptide serums after hair transplant, and red light therapy after hair transplant belong below the basics. Optional recovery ideas should never become more important than the quality of the operation.
A possible future place for topical metformin
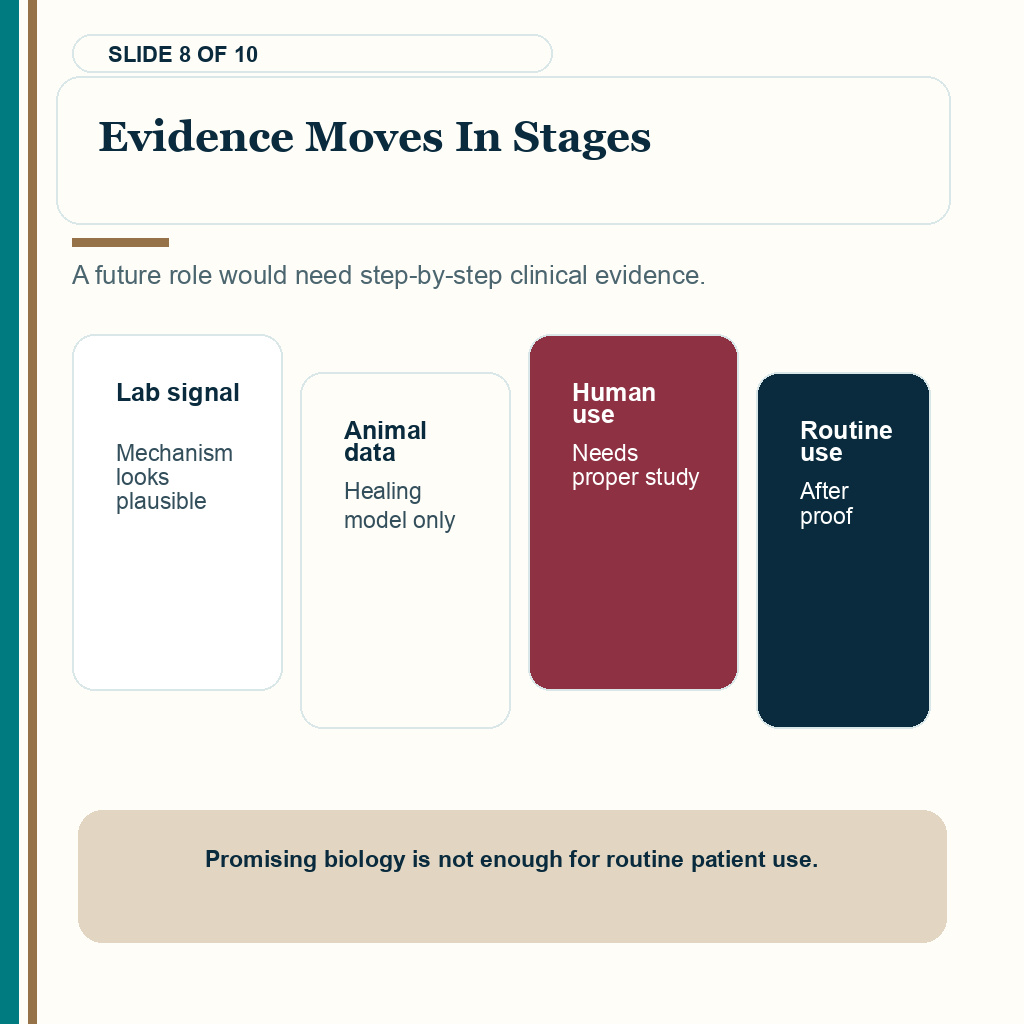
If topical metformin becomes useful in hair transplant recovery, I would expect it to be tested in a controlled way. That is a different question from established hair medication timing, such as minoxidil after hair transplant. The basics would include a defined concentration, a defined base, clear timing after FUE, use only after appropriate skin closure if that is the safe route, documented donor photography, side effect tracking, infection tracking, pigmentation review, scar visibility scoring, short hair donor assessment, and longer follow up.
The most realistic early role would be donor skin healing quality, not a promise that extracted follicles come back. Even that needs direct human evidence. It would also need clear exclusions for irritated skin, allergy, active infection, open wounds, poor hygiene, uncontrolled diabetes, inflammatory scalp disease, or difficulty following aftercare.
That kind of evidence would be useful. It would help surgeons decide whether the product adds anything beyond careful extraction, correct washing, and time. Until then, it remains a discussion point, not a standard part of a FUE recovery protocol.
Protect the donor area with proven steps first
You can protect the donor area in ways that already matter. Follow the washing protocol. Do not scratch. Avoid unnecessary friction. Keep hats, pillows, helmets, and exercise timing sensible. Send photos early if there is redness, bumps, pain, fluid, wet crusting, or unexpected scabbing. If a product causes burning, new itching, more redness, wet crusts, or bumps, stop and ask before layering another product over it.
If the donor area looks patchy early, that does not prove permanent damage. Hair length, shock loss, scabs, inflammation, lighting, and haircut length can change the appearance. A patchy donor area after hair transplant needs timing and photos before anyone judges the final donor result.
If the concern is visible dots with short hair, the better discussion is donor extraction quality, hair caliber, skin contrast, punch size, spacing, and haircut expectations. Short hair after FUE donor scars is closer to that question than any single cream.
The first donor area priorities are closure, cleanliness, photo review, and avoiding unnecessary irritation.
What is my current position on topical metformin after FUE?
I understand the interest. Everyone wants the donor area to heal cleanly, look normal with short hair, and preserve future options. But a hopeful topical product cannot compensate for poor extraction, excessive graft numbers, weak donor selection, or unrealistic planning.
If you are booked for FUE and want to use topical metformin, tell your surgeon before surgery. If surgery is already done, do not apply it to fresh donor skin without review. Share the ingredient list, prescriber or source, timing after surgery, and current donor photos, then ask whether the timing is appropriate. If the skin is irritated, infected, open, painful, wet, or worsening, stop experimenting and get examined.
My current position is strict because the donor area is limited. I am not rejecting research. I am protecting the donor area. Topical metformin may become interesting for donor skin research, but it should not be treated as proven donor regrowth after FUE. Protect the donor area first. Choose a surgeon who plans extraction responsibly. Then judge new recovery products only when the evidence, timing, and skin condition make sense.