


Scalp Cyst Before FUE Needs Mapping First
A scalp cyst is not always a reason to cancel a hair transplant. A small, quiet, stable pilar or epidermoid cyst may sometimes be mapped and worked around. An inflamed, painful, draining, recently squeezed, or poorly diagnosed lump is different. With that kind of skin change, I would pause the surgery plan until the area is understood and settled.
Size alone does not answer this. I look at the exact location, the skin over the lump, recent change, tenderness, and whether it sits in the donor area, recipient area, or crown transition zone.
Quiet skin and active skin do not carry the same surgical risk. Quiet skin can sometimes be planned around. Active, open, infected, or recently treated skin can make graft placement and donor harvesting less predictable.
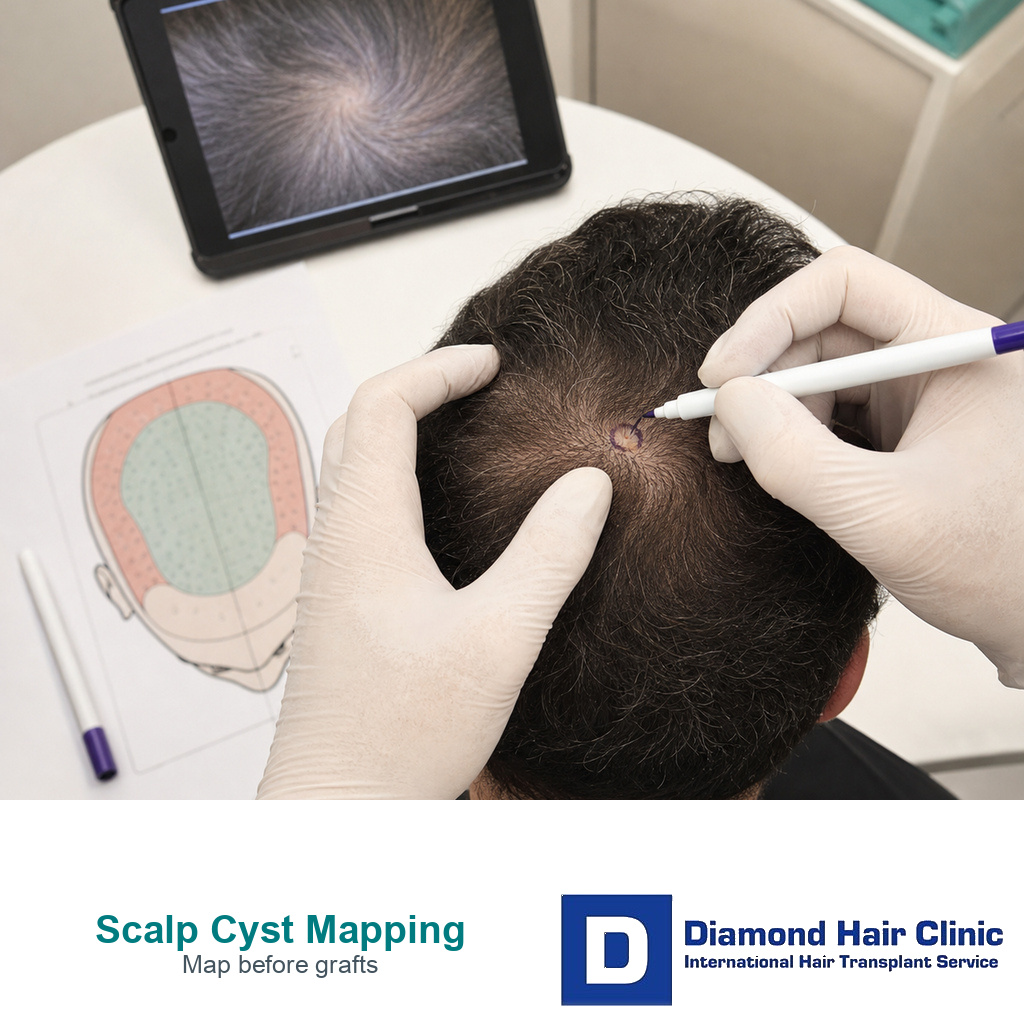
Scalp cyst surgery map
Map the cyst before graft numbers
I first place the lump on the surgical map. Then I decide whether the skin is quiet, active, uncertain, recently opened, inside the working zone, or already changed by removal.
Mapping check
A calm cyst still has to be placed on the surgical map
Long history, no pain, normal skin, no drainage, no recent swelling, and a clear location.
Send daylight photos from above, both sides, and close range without pressing the lump.
Equal density through the raised point before the tissue and location are reviewed.
A quiet cyst may be worked around only after it is marked against the donor and recipient plan.
Cyst details matter before graft numbers
A small lump on the crown or donor scalp can create a lot of worry when surgery is already booked. Some people fear that the lump will block blood flow or damage the transplant. I do not answer that from a written description alone. I first map the lump against the planned hairline, crown pattern, and donor harvest zone.
A scalp cyst is often a pilar cyst, also called a trichilemmal cyst, or an epidermoid cyst. These are usually benign skin lesions, but the transplant plan still has to respect them. A cyst wall, an old inflamed pocket, or a removal scar can change the local tissue. That matters when we are trying to place grafts evenly and protect blood supply.
Not every cyst needs to be removed before FUE. The question is whether it is quiet enough to map around, whether it sits inside the working zone, and whether there is any diagnostic uncertainty. A small stable lump outside the graft field is a different problem from a painful or changing lump exactly where donor harvesting or graft placement is planned.
Start with evidence, not pressure to keep the date. Send clear daylight images from above, both sides, and close range. If the lump can be gently pointed out without pressing it, that helps. If the lump is pigmented, changing, crusted, bleeding, or not clearly a cyst, I treat it more like a skin lesion question. That makes the logic closer to scalp moles before hair transplant, where diagnosis comes before graft numbers.
A cyst before surgery should not be confused with ordinary postoperative pimples. If you already had surgery and now see small bumps, the review is closer to redness, scabs, and pimples after hair transplant or bumps and ridges after hair transplant. A lump already present before surgery belongs in the surgical plan before surgery starts.

Use the 8 scalp cyst planning slides below to separate location, activity, mapping, change history, timing, useful details, donor safety, and direct review. Swipe sideways, use the arrows, or choose a number below the image.

A quiet cyst can sometimes be worked around
A small cyst that has been present for a long time, is not tender, and has normal skin over it may be compatible with surgery in selected cases. That does not mean I ignore it. It means the plan is adjusted around a known point on the scalp.
If the cyst is in the donor area, I may change the punch distribution so grafts are not harvested through poor tissue. If it is in the recipient area, I may avoid placing grafts directly into the raised or scarred zone until the skin is stable. If it is near the crown, I consider whether the cyst changes the visual density plan or whether a small zone should be left untouched.
Working around a cyst is not the same as promising equal density through it. Healthy skin matters more than forcing grafts into a questionable point. A tiny avoided zone can be safer than spending grafts in tissue that may not heal predictably.
This is where donor judgment matters. If the donor is already limited, I do not waste grafts chasing a cosmetic problem created by a cyst. I compare the plan with broader donor safety principles such as donor miniaturization and safe zone planning before deciding how much correction is realistic.
A cyst can delay surgery
An inflamed cyst is a different problem. Redness, warmth, pain, discharge, crusting, recent swelling, or repeated drainage means the skin is active. I do not want to place grafts through inflamed skin, and I do not want donor harvesting to pass through a recently infected area.
Warm compresses, antibiotics, local drainage, or dermatology treatment may be appropriate before travel, but those steps are not a green light by themselves. The scalp still has to be judged again before surgery. A recently drained cyst can still have irritated tissue, an open puncture point, or a capsule that may flare again.
If the cyst is painful or draining, surgery planning should pause. The priority becomes diagnosis, infection control, and skin recovery. This is similar to the way I treat active scalp infection. A page such as tinea capitis and hair transplant explains the same principle in another condition. Treat the active scalp problem first, then plan grafts.
Antibiotics can also complicate the conversation. They may calm inflammation, but they should not be used to push an uncertain scalp into surgery. If antibiotics are already being used, I review why they were prescribed, whether drainage was present, and how the skin looks now. That sits close to the logic in antibiotics before hair transplant.
Squeezing a cyst before surgery can create risk
Squeezing, lancing, or scraping a cyst at home because surgery is coming soon is one of the easiest ways to make the plan less safe. It may feel like a quick fix, but it can turn a stable closed lump into irritated skin, drainage, bruising, or infection risk.
A cyst often has a wall or capsule. Emptying the contents without proper removal can allow recurrence. More importantly for FUE planning, home drainage creates a wound in the exact skin I need to judge. A small quiet cyst is easier to plan around than a recently damaged area with uncertain healing.
I also avoid dramatic promises after cyst removal. Removal can be sensible when the cyst is large, recurrent, painful, or in the way of the transplant plan, but removal leaves a scar. A scar can be grafted in selected cases only after the tissue matures and the expectation is realistic. It is not a shortcut for surgery day.
For that reason, send images before travel. If the lump looks active, local dermatology review may need to come first. If it looks quiet and outside the graft field, surgery may still be possible with mapping. That difference should be clear before flights, hotels, and graft numbers are locked in.
Cyst removal before transplant depends on the case
Removal makes sense when it gives safer skin to work with. If a cyst is repeatedly inflamed, growing, painful, uncertain, or placed exactly where grafts are needed, removal may be the better first step. If it is tiny, quiet, and outside the working area, removing it just before surgery can create more disruption than benefit.
The timing matters. Fresh cyst removal can leave swelling, stitches, scabbing, or a scar that is not ready for dense grafting. If removal is needed, I usually want enough healing time for the skin to settle before judging density. That may mean delaying the hair transplant instead of forcing grafts into a recovering wound.
The scar after removal becomes part of the plan. A linear or round scar in the donor area may reduce harvestable surface. A scar in the recipient area may need lower density, staged grafting, or no grafting if the tissue is not suitable. The correct plan is built around the final healed skin, not the cyst alone.
This is also separate from inflammatory scalp diseases such as scalp psoriasis and hair transplant. Psoriasis changes a broader skin field. A cyst is usually a local point. Both need respect, but the surgical decisions are different.

Postoperative bumps differ from a cyst before surgery
A bump after surgery needs a different review from a lump that was already present before surgery. It might be folliculitis, an ingrown hair, local irritation, retained crust, or a lesion that behaves like a cyst. Timing, location, pain, drainage, and response to treatment all matter.
If bumps appear after grafting, I look for patterns. Multiple small pustules are often closer to folliculitis after hair transplant. Tiny pale spots or plugs may be closer to white spots after FUE. One larger persistent lump needs a more specific review.
Do not pop it aggressively. Share clear close range images. Tell the clinic when it started, whether it is painful, whether anything drained, and what treatment has already been used. If there is fever, spreading redness, worsening pain, or heavy discharge, local medical review should not wait for a cosmetic follow-up.
Useful cyst information should be sent before booking
Clearance should be based on evidence, not a short description. Send current scalp photos, the exact location, any growth or drainage history, diagnosis or previous removal notes, and current medicines or antibiotics. If treatment happened recently, include the date and what was done.
I also compare the cyst with the overall candidacy picture. Strong donor hair, a quiet cyst away from the donor path, and realistic goals are different from weak donor hair, active inflammation, and pressure to finish everything in one trip. That broader judgment is part of being a good candidate for hair transplant.
After surgery, the same honesty continues. If bumps, redness, tenderness, drainage, or a persistent lump appears, the recovery plan should respond to the skin rather than rely on hope. General hair transplant recovery instructions help, but a persistent lump needs specific review.
What should be clear before travel?
A scalp cyst before hair transplant is neither a routine danger nor a detail to ignore. A quiet, stable, clearly mapped cyst may be worked around. An inflamed, draining, recently squeezed, rapidly changing, or poorly diagnosed lump can delay surgery. A removed cyst may leave scar tissue that needs its own plan.
Treat the cyst as part of the surgical map, not as an afterthought. Before travel, I want the location, diagnosis, skin activity, treatment history, and surgical plan clear enough that the graft plan can respect the skin that is actually there. That protects the donor area, the recipient design, and the long-term result better than a rushed decision.