CCCA and Hair Transplant Planning
With central centrifugal cicatricial alopecia, surgery belongs later in the conversation, after the scalp disease is quiet and donor reserve is safe. CCCA is not ordinary female pattern thinning, because this is not only a density issue. It is an inflammatory scarring process that can destroy follicles.
If someone with CCCA wants grafts in the crown, the first decision is not a graft number. The diagnosis, flare history, treatment record, and clear photos should show whether the center of the scalp is stable. Active CCCA is a reason to wait, not a reason to rush surgery.
CCCA changes the first question
CCCA usually affects the center or crown of the scalp first. It is seen more often in Black women, but the surgical issue is not ethnicity alone. The issue is scarring inflammation. Once follicles have been replaced by scar tissue, medicine and surgery both become more limited.
CCCA is separate from the usual conversation about female hair transplant candidacy. A woman with stable pattern thinning and strong donor hair is a different surgical situation from a woman with central scarring, tenderness, scale, burning, or a history of scalp injections and dermatology treatment.
It also differs from a pure hairline request. Female hairline transplant planning is about shape, direction, and facial balance. CCCA is usually about whether the crown skin is safe enough to receive grafts at all.
The diagnosis must be clear before graft planning
The first consultation should clarify whether a dermatologist has confirmed CCCA, whether a biopsy was done, and what other diagnoses were considered. Traction alopecia, female pattern loss, seborrheic dermatitis, telogen shedding, and other scarring alopecias can overlap in a real patient. A crown that looks thin from breakage or traction is not the same surgical problem as a scarred central patch with lost follicular openings.
The diagnosis changes the surgical question. In traction alopecia hair transplant planning, the main issue is often whether the pulling has stopped and whether the hairline skin is healthy enough. In CCCA, I am usually looking at central scalp scarring, treatment stability, and whether inflammation has truly stopped moving.
The disease should not be treated as the patient’s fault. Hair practices can contribute to irritation in some people, but many patients have done everything carefully and still develop CCCA. The surgical plan should stay respectful and evidence based.
That respect matters in consultation. If a patient has been told for years that styling explains everything, she may arrive feeling dismissed before the scalp is even examined. The history should include braids, relaxers, wigs, heat, and tight styles because they can affect irritation and traction. Those answers are not there to shame the patient. They help show whether avoidable scalp stress should be reduced before surgery is even considered. For that part of planning, see chemical relaxers and hair transplant timing.

CCCA planning starts with diagnosis and stability before any graft number is discussed.
A quiet photo is not the same as stable disease
One quiet day can be misleading. A scalp can look quiet in a photo and still flare again after treatment changes, stress, illness, styling pressure, or no obvious trigger at all. The trend matters more than one image.
In many scarring alopecia discussions, a year of stability is treated as a serious benchmark. That is not a magic certificate, but long stability is much safer than recent improvement. A few quiet weeks after stronger medication are not enough proof for a surgical plan. I also separate a scalp that is quiet only while treatment has just been intensified from a scalp that stays predictable after the plan has settled.
The same caution appears in scarring alopecia and lichen planopilaris. Different diseases can share one surgical rule. Active inflammation should be controlled before donor hair is spent.
Medication timing also needs to be clear. If the dermatologist has just changed treatment, the scalp may look temporarily quieter while the true trend is still unknown. Surgery should not be scheduled simply because the most recent photo looks better. The treatment plan, symptoms, and scalp surface should all stay predictable before surgery enters the discussion.
Donor hair should not be wasted on unstable skin
Every graft taken from donor reserve is a limited resource. If the recipient scalp is still inflamed or scarred in a way that cannot support growth, the patient can lose precious donor reserve without gaining a useful cosmetic improvement.
I examine the donor area carefully before saying yes. I look at hair caliber, density, miniaturization, scalp health, prior extraction scars, and the amount of reserve that must be protected for the future.
If the donor is already weak, CCCA makes the decision stricter. A patient with a weak donor area cannot afford an optimistic experiment in poor recipient scalp. The safer answer may be medical control, camouflage, or no surgery for now.
This donor conversation can be difficult because the crown is the area the patient sees and feels every day. Still, donor reserve is what makes any future repair or second stage possible. If the first plan spends too many grafts chasing a scarred crown, there may be little left for a more useful correction later.
Graft survival may be lower in scarred scalp
Scarred scalp is not the same as normal crown skin. Blood supply, tissue stiffness, inflammation history, and loss of follicular openings can all affect how grafts behave. Normal survival or normal density should not be promised in a scarred CCCA area.
When surgery is reasonable, the plan may be smaller and use lower density than the patient expects. The first goal may be a modest softening of the visible patch, not complete coverage. How surgeons calculate graft numbers explains normal graft planning, but CCCA adds disease stability to that calculation.
A low density plan can be the safer plan. It may protect the skin and donor area better than trying to force thick coverage into tissue that cannot support it.
I explain this before surgery because disappointment often comes from a mismatch between hope and tissue biology. If the patient expects normal crown density, a cautious plan can feel too small. If she understands that the first aim is safe improvement in scarred skin, the same plan may feel more reasonable.
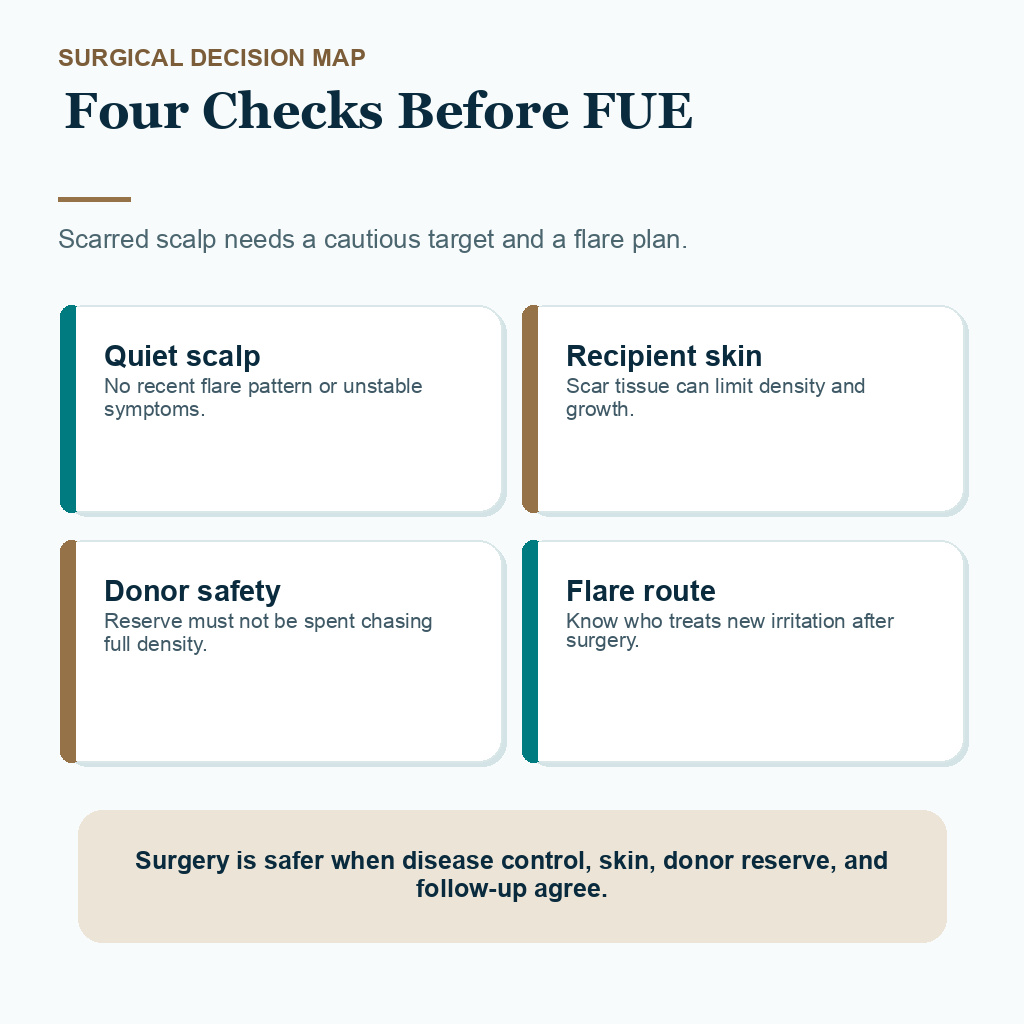
The safer decision checks disease control, scarred skin, donor reserve, and the flare plan together.
A staged decision sequence
When a patient might be a candidate, I use a staged decision. The order protects the patient from turning a chronic scalp disease into a failed transplant story.
The sequence starts with disease control rather than graft numbers. I want a confirmed diagnosis, a quiet scalp, dermatologist involvement, enough donor reserve, and a modest target area before I treat FUE as an option. If the disease is still active, if the goal depends on dense crown coverage, or if the patient is not prepared for lower graft survival in scarred skin, waiting or not operating is safer than forcing surgery.