


Hair Transplant Case Pages Need Real Surgical Context
A useful hair transplant case should show the thinking behind the result, not only the change in the photos. If you are comparing clinics from another country, a case page should help you understand why the plan was chosen, what was protected, and what should not be copied from that result. The point is not to find a twin. It is to see whether the reasoning could apply to your donor area, hair loss pattern, and long-term plan.
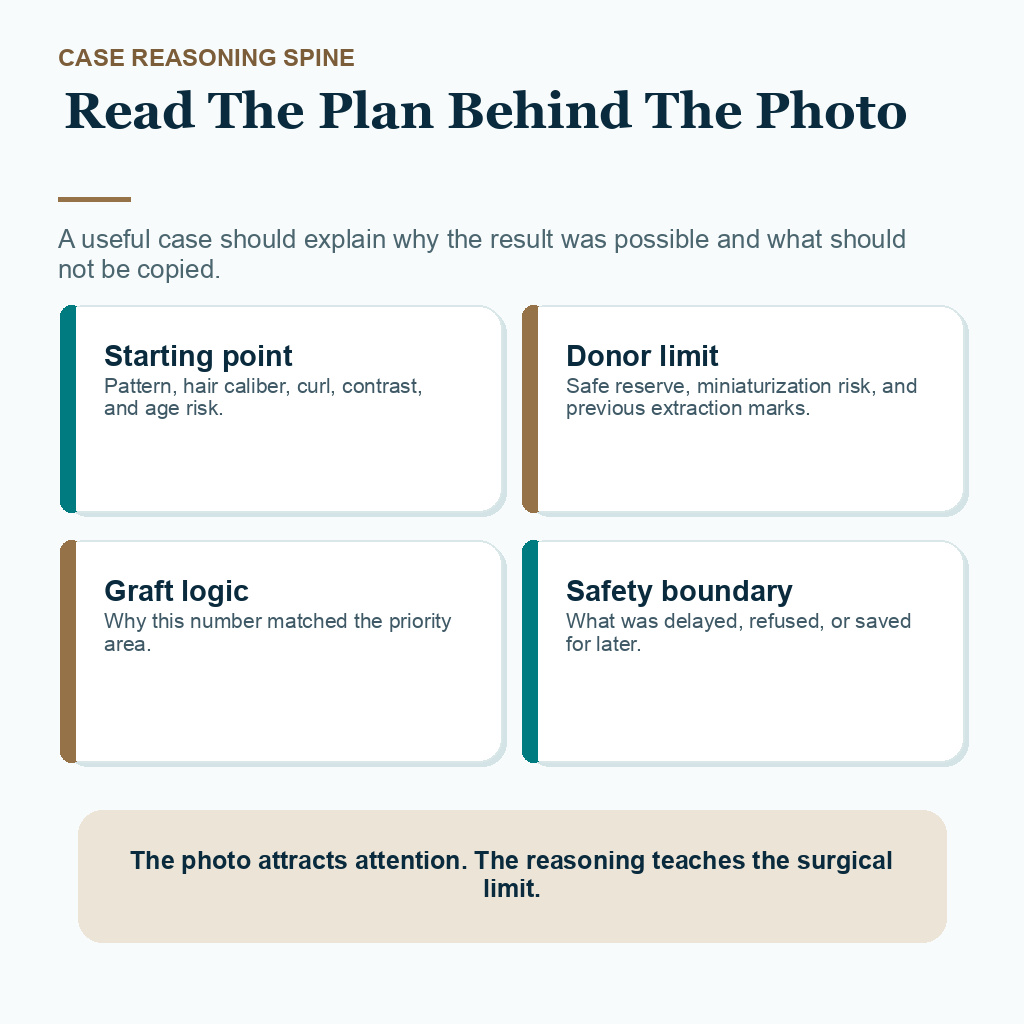
Use this page as a guide for reading Diamond Hair Clinic cases as the library grows. Each case should explain the hair loss pattern, donor limits, graft choice, safety boundary, and photo conditions. A photograph can show that a result happened. The reasoning explains whether that result is relevant to your donor area, your hair characteristics, and the result you are hoping for.
Before trusting any hair transplant before and after photos, ask a harder question. Does this case explain the decision, or does it only show a transformation?
A useful case should explain the reasoning
A useful case starts with the visible pattern, but it should not stop there. Hairline shape, crown demand, hair caliber, curl, skin contrast, age range, medical context, previous surgery, donor strength, and future hair loss risk all change the meaning of a result.
The case should also explain the main decision. Was the goal to rebuild the frontal third, soften the hairline, improve the crown, repair a previous result, or protect donor reserve for later? Without that context, the result can be easy to admire and hard to use.
Compare results from hair like yours, not only results with the same Norwood label. Similar hair loss on a chart does not mean the same donor strength, hair shaft thickness, curl behavior, contrast, or surgical plan.
The notes behind the photos matter
When I evaluate a case, the most important details are often the details a gallery does not show. Family pattern, medication use, hair caliber, curl, contrast, miniaturization in the donor area, previous extraction marks, crown risk, and expectations all change the plan.
A case page should not only say how many grafts were used. It should show which facts pushed the plan forward and which facts made me slow down. This matters in Turkey comparisons because two photos that look similar can hide very different donor situations. If those notes are missing, I treat the photo as incomplete.
Do not stop at, “Do you have someone like me?” Ask whether the clinic can show how the plan was chosen, what was protected, where the limit was, and why that same plan may or may not fit your donor area.
The same Norwood pattern does not mean the same graft number
The Norwood pattern helps describe the shape of male hair loss, but it does not decide the safe graft number by itself. Two men can both look like Norwood 4 from the front, while one has strong donor density and the other has early donor miniaturization, wider crown demand, or fine hair that gives less coverage per graft.
The graft number should come from the medical plan, not from matching another person’s number. When I read a case, I need to know what area was prioritized, what was left alone, and why the number was chosen. A 2,800 graft plan can be more responsible than a 4,200 graft plan if the larger number spends donor hair that may be needed later.
Graft package marketing needs a surgical explanation. A person comparing price or package numbers should also understand why price per graft can mislead hair transplant patients when donor limits and long-term planning are not explained.
These 8 case reasoning slides separate the photo from the plan, starting point, Norwood label, donor budget, graft number logic, photo conditions, waiting or refusal, and follow-up context. Swipe sideways, use the arrows one slide at a time, or choose a number below the image.


Donor quality can limit a case
A case should make donor capacity visible in the explanation, even when the donor photos are not shown in close detail. I look at density, hair shaft thickness, safe zone stability, miniaturization, previous extraction marks, skin contrast, and the likely future demand from untreated areas.
Some people can safely support a fuller frontal plan. Others need a smaller design, staged planning, medical stabilization, or no surgery. In those cases, I am not trying to make the result smaller. I am trying to avoid creating a donor problem while solving a coverage problem. Donor hair is a limited surgical budget. Once it is spent poorly, repair becomes harder.
A strong result from another person can still be irrelevant if the donor supply is different. A weak donor area changes the interpretation of even attractive case photos.
A lower graft number can be the safer plan
A higher graft number does not make the operation stronger by itself. Sometimes a lower number is the more responsible decision because it keeps the donor area usable, avoids chasing thin crown coverage too early, or leaves enough reserve for future loss.
If the donor supply is strong and the target area is limited, a larger session may be reasonable. If the donor is average, miniaturized, scarred, or already used in a previous surgery, the better plan may be smaller, staged, or delayed.
A useful case explanation should make that choice visible. It should say why the number was enough for the goal, why more grafts were not taken, and what would have made a bigger session unsafe.
A case should not promise a copied result
Every case should say what was not promised. A mature hairline case should not imply a teenage hairline. A frontal restoration case should not imply full crown coverage if the crown was deliberately left for later. A repair case should not imply that every bad result can be fully reversed.
The boundary should be visible before the photo is trusted. A case becomes more useful when it explains the limitation. That may mean lower density than first requested, a higher hairline, staged crown work, or a decision to protect donor reserve instead of chasing maximum coverage.
The same boundary matters if the graft number changes on surgery day. The reason should be medical, visible, and explained before the plan continues.
Some cases should wait or be declined
A real case library should not only show successful operations. It should also teach what would have made surgery unsafe or unwise. Unstable hair loss, poor donor quality, unclear diagnosis, active scalp disease, unrealistic density expectations, a hairline request that will not age well, or a repair plan that would spend the last useful donor reserve can all change the answer.
Sometimes the next step is medication, better photographs, blood or scalp evaluation, waiting for stability, or a smaller design. Sometimes the responsible answer is no.
A surgeon may have clear reasons to decline hair transplant surgery when the plan would harm the person later. A refusal can protect the donor area, the hairline, and the options that remain.
Refusal cases should also be visible
Cases where surgery is delayed or declined often teach more than dramatic photo results. They show where the safety line sits.
Someone may need to wait because the hair loss is unstable, donor reserve is too weak, the diagnosis is not clear, the requested hairline would look unnatural later, or a repair plan would consume too many grafts for too little benefit. Another person may need better photos, scalp evaluation, medical treatment, or a simpler plan before surgery becomes reasonable.
For someone traveling internationally, a clear delay can be a trust signal. A clinic that can explain why surgery should wait is showing more clinical responsibility than a clinic that tries to turn every inquiry into an operation.
Photos should be read with context
Photos can help, but they are not promises. Lighting, angle, hair length, styling, wet or dry hair, camera distance, scalp contrast, and follow-up month can change how dense a result appears. A strong photo should still be read with caution.
Each case should explain what the photo can show and what it cannot show. It may show hairline softness, frontal framing, improved coverage, or donor healing. It cannot prove that another person will get the same density, same hairline, same healing, or same future stability.
Repair cases need the details read together. Pluggy grafts, wrong direction, scarring, overharvesting, and grafts with multiple hairs in the hairline must be read together with the repair limit. The broader repair logic is explained in bad hair transplant repair planning.

Photos become more useful when the case explains what the image cannot show by itself. The same caution applies to any hair transplant plan from photos, because photos can start a consultation but should not finish the surgical decision.
International patients need a disciplined comparison
If you are comparing clinics from another country, do not stop at “Do you have a result like mine?” Ask what the donor allowed, why the graft number was selected, what area was left untreated, and what would have changed the plan on surgery day.
Also ask who evaluates donor capacity, who designs the hairline, and who decides whether surgery should be smaller, staged, postponed, or declined. The answer matters because the most important decision is often made before the first graft is extracted. I explain that decision sequence before travel in case review before travel.
A case page is stronger when it lets you see that reasoning without needing to guess. It should help you compare the doctor’s method, not only the clinic’s photography.
Each case page should contain the clinical reasoning
Each case should have the same basic clinical spine. It should explain the pattern, donor limit, reason for the graft number, priority area, areas intentionally left untreated, safety boundary, photo timing, and what was not promised.
For example, a frontal hairline case should say whether the crown was ignored, deferred, or not suitable for coverage. A crown case should explain why density expectations are different from the front. A repair case should explain the previous problem, available donor reserve, and risk of making the donor or hairline worse.
The library should grow deliberately. A smaller number of clearly explained cases is more helpful than many photographs with no reasoning attached.
The case entry format that protects context
A real case entry should keep the structure consistent so the patient is not left guessing from photos alone. The case should make the clinical boundary visible before the result is judged.
- Pattern and starting point records the visible hair loss pattern, recipient priority, hair characteristics, and the problem the patient wanted solved.
- Donor limit explains the donor strength, hair caliber, safe extraction boundary, miniaturization risk, or previous extraction concern that shaped the plan.
- Graft decision shows why the graft range was chosen, why more grafts were not taken, and which area had priority.
- What was not promised names crown coverage, exact density, a copied hairline, repair perfection, or any result the donor area could not support safely.
- Unsafe boundary describes the finding that would have reduced the plan, delayed surgery, or made surgery the wrong decision.
- Photo reading explains lighting, hair length, angle, styling, timeline, and what the image cannot prove for another patient.
If one of these details is missing, I treat the case as incomplete. It may still be an interesting photo, but it is not enough to guide a surgical decision.
What should follow-up add to a case page?
A case page becomes more useful when follow-up is part of the reasoning, not only a final photo. The reader should know when the result was photographed, what stage of growth it represents, whether the donor healed normally, and whether the patient had continuing native hair loss behind the transplanted area.
Follow-up also explains what was not claimed. A case may show a strong frontal frame without promising full crown density. It may show scar camouflage without promising that every scar disappears. It may show improvement after repair while still protecting the remaining donor reserve.
Explained cases are more useful than transformation galleries because they show the thinking behind the result. The photo attracts attention, but the reasoning teaches the patient what can and cannot be copied.
The library should grow through explained cases
When real cases are added, each one should answer the same clinical questions in plain language. What was the pattern? What did the donor allow? Why was that graft number chosen? What was left untreated? What was not promised? What would have made surgery unsafe? How should the photos be read?
A patient photo belongs here only when consent and educational use are clear. The case should not expose private details, and it should not turn the person into an advertisement. The purpose is clinical understanding, not pressure.
If you are still comparing clinics, ask who makes the plan and whether the clinic can explain the same level of reasoning behind the cases it shows. A clinic should be able to show how surgeon involvement changes the hair transplant plan, not only display attractive photos. If the plan still feels unclear, a second opinion before hair transplant surgery can prevent a decision based only on appearance.