


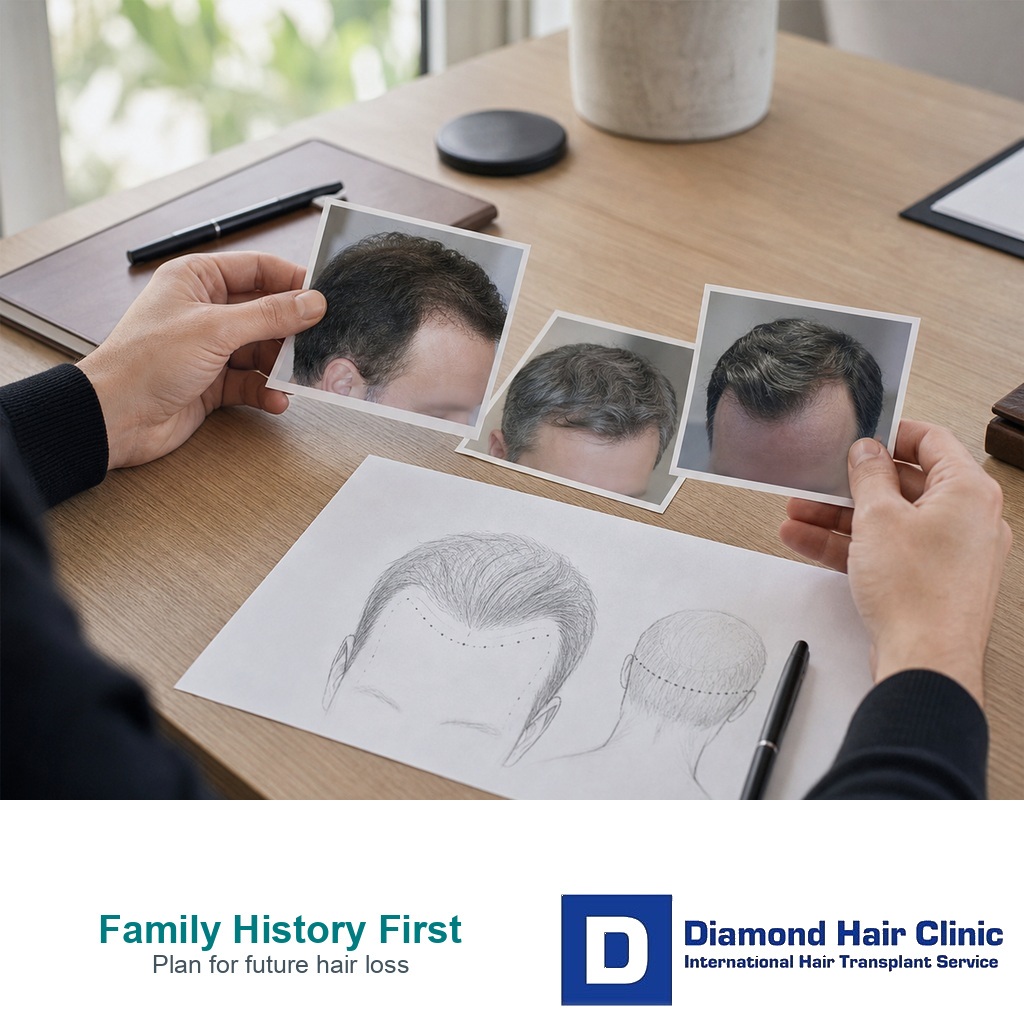
Family Hair Loss History and Transplant Planning
A strong family history does not give me a fixed map of your future, and it does not rule out surgery by itself. It changes the safety margin. If your father, brother, uncle, or grandfather became very bald, I need to be more careful with hairline height, graft spending, crown timing, and donor reserve.
Family history is a warning light, not a verdict. I still examine your current hair, donor density, miniaturization, age, medication tolerance, crown condition, and expectations. In Norwood 3 hair transplant planning, the first operation can define what is still possible later.
The common mistake is reading family history in only one direction. You may panic because every male relative became bald, or you may ignore risk because your hair still looks good today. Both reactions can lead to poor timing. The useful question is what the family pattern should change in the design.
Family details that matter before surgery
Pattern hair loss is linked to genes and androgen sensitivity, and the visible pattern often affects the front, temples, mid scalp, and crown over time. Family history gives me a clue about where your hair may become weak, how early it may progress, and how wide the final balding zone may become. It is never the only clue.
During planning, I ask about both sides of the family. The mother’s side matters, but so does the father’s side. I want to know who lost hair early, who kept a stable mature hairline, who developed crown loss, and who reached advanced baldness. If close relatives reached advanced loss in their twenties or thirties, I use more caution than I would for an older patient with long stable temple recession.
The old idea that only the mother’s father matters is too narrow for surgical planning. Repeated patterns across the family matter, but your own scalp exam carries more weight than any family story.
Female relatives matter too, especially when thinning is diffuse rather than a simple Norwood pattern. A mother, sister, aunt, or grandmother with a widening part, crown thinning, or long term density loss can change how I read the risk. In women, I also want medical causes such as thyroid imbalance, iron deficiency, postpartum shedding, medication changes, or signs of androgen excess considered before a transplant plan is treated as cosmetic only.
Age changes the level of caution. A young person with strong family baldness and active miniaturization needs the same careful review I use when I assess being too young for a hair transplant or having surgery while hair loss is still active. The family pattern does not decide alone. It changes how strictly I read the other findings.
Family history does not predict the future pattern exactly
Family history can suggest the direction of risk. It can show that crown loss runs strongly, that temple recession starts early, or that several men in the family move beyond an ordinary mature hairline. It can also show a wide range of outcomes inside the same family, which is why I do not copy one relative’s head and treat it as your future.
The limitation matters. Brothers can age differently. A father may lose hair early while a son keeps stronger density, and the reverse can happen too. Lifestyle, age, medication use, medical history, and the biology of your own follicles all matter. I use family history to widen or narrow the safety margin, not to promise a final Norwood class.
Family history works best when it is compared with the current scalp exam, not when it is treated as a fixed prediction.
The practical distinction is simple. Family history tells me where risk may go. The scalp exam tells me what is already happening now. Surgery should be planned from both, because I need to know how much stable donor hair can be used without creating a future shortage.
Father or brother pattern can be useful without being copied
I separate three things. Age of onset, final extent, and current similarity. If your father was Norwood 6 by 35, that carries more planning weight than a relative who developed mild crown thinning after 60. If your older brother has the same early temple recession and crown thinning that you now show, I take that more seriously than a distant relative with a different pattern.
Clear, dated photographs help more than family labels. A photo of your father at 30, 40, and 50 can tell more than the sentence “my father is bald.” Comparisons at the same age are especially useful. I also ask whether relatives used finasteride, minoxidil, wigs, fibers, or previous transplants, because those can hide the natural pattern. The consultation needs facts, not family legend.
If your own pattern is still mild but your family pattern is aggressive, the plan leans conservative. If your family history is severe but your age and scalp exam show long stability, the decision can be more flexible. The key is that family history adjusts the safety margin. It does not replace what I see under magnification.
Strong family baldness can make surgery too early
Surgery becomes too early when the future pattern is likely to outrun the current design. At 22, early temple recession with diffuse mid scalp miniaturization, a father and brother with advanced baldness, and no sign of stabilization needs a different conversation from a stable 36 year old with a strong donor area and a limited frontal pattern.
The danger is not that transplanted grafts disappear. The danger is that native hair around the grafts continues to thin, leaving a dense low hairline in front of a weak mid scalp or crown. That can look unnatural and can force expensive repair decisions. It also spends grafts that may be needed later.
In this setting, waiting can be a medical planning decision, not a refusal. I may ask for serial photographs, trichoscopy, medication review, and a follow up interval before surgery. I am looking for evidence. Are photos taken under the same lighting changing? Is miniaturization widening under magnification? Is the crown or mid scalp weakening during observation? If progression is clear, the operation may need to become smaller, later, or more conservative. Planning a hair transplant in your 30s often has a different balance from surgery in the late teens or early twenties.
Hairline design should change when future loss is likely
A strong family pattern usually makes me raise the hairline slightly, soften the temple angles, and avoid closing the temples too aggressively. A low teenage hairline can look tempting in the mirror, but it can become a graft trap if the mid scalp and crown thin later. The design must still look natural when you are older.
For hairline work, I look for mature height, soft irregularity, and density placed where it will age well. In family pattern cases, hairline design in hair transplant has to sit inside the donor budget. A hairline is not a drawing on a forehead. It is a long term use of a limited donor supply.
A conservative hairline is not a weak result. It is a way to preserve naturalness if future hair loss becomes stronger. The opposite error is spending too many grafts on a low front and then having no good answer when the crown opens.
Crown coverage needs extra caution
The crown can absorb many grafts because of the swirl, the wide surface area, and the way light exposes thin density. In a strong family crown pattern, early crown coverage can use grafts that may later be needed to connect the frontal zone, reinforce the mid scalp, or preserve a natural overall frame.
If the crown is mild and the front is the main concern, I may delay crown work and protect donor reserve. If the crown is the main visible problem and the front is stable, the plan can shift. The sequence matters, and choosing hairline or crown first depends on age, donor strength, future loss risk, and what bothers you most.

A strong family pattern often means using fewer grafts in the crown early and keeping the frontal design mature.
The crown is where overpromising is common. It is understandable to want the swirl filled because it appears in photos and under bright light. I still have to protect the same grafts you may need in ten years. In advanced family patterns, crown expectations need careful wording before any graft count is accepted.
Finasteride and minoxidil in family pattern planning
Medication does not change your genes, but it can change the speed and visibility of progression in suitable patients. Finasteride can help protect miniaturizing native hair for some men, and minoxidil can support density in selected areas. These medicines require proper medical discussion, side effect review, and realistic expectations.
When family history is strong, I pay close attention to whether native hair can be stabilized before surgery. A good response to medical treatment may make the surgical plan less exposed to rapid ongoing loss. If you cannot or do not want to use medication, surgery may still be possible, but the design has to be more conservative.
Medication review, including finasteride before and after hair transplant and minoxidil after hair transplant, can affect how aggressively the graft plan is designed. Medication review comes before the design is fixed, especially when family history suggests future spread.
Mixed or unknown family history is still useful
Mixed family history is common. One side may show early baldness, while the other side keeps strong hair into older age. That does not cancel the risk. It means I need to judge your actual scalp more carefully and avoid making a plan from one convenient relative.
If family history is unknown because of adoption, limited contact, or missing relatives, I rely more heavily on serial photos, trichoscopy, donor examination, and the current speed of change. Unknown history does not make the plan risk free. It simply removes one clue.
This is the opposite mistake from panic. No known family history does not prove safety, especially if your own scalp already shows miniaturization. Severe family history raises caution, but weak or unknown family history does not erase the need for diagnosis.
When the evidence conflicts, I protect the donor supply before spending it aggressively. Uncertain future loss needs reserve. It is easier to add density later than to repair a low, isolated hairline that used too many grafts while the donor area is weak.
Donor quality changes the decision
Family history tells me how much future demand may appear. Donor quality tells me what supply is available. Those are separate questions, and both matter.
Thick caliber, good density, and a stable safe zone give more room. Weak donor density, miniaturization near the donor margins, retrograde thinning, or previous overharvesting makes the plan tighter. If several relatives developed thinning above the ears, in the nape, across the sides, or inside what should look like the permanent rim, I do not assume that the whole back and sides are equally safe. I check miniaturization inside the donor and near the margins before deciding extraction density.
A family pattern that reaches advanced baldness with a narrow donor rim can turn an impressive first graft number into a later shortage. I connect family history with lifetime hair transplant graft planning because the first operation must not steal from the second or third decision.
When donor density is weak, weak donor area hair transplant can become the more important question than the family pattern itself. The donor exam can turn a possible operation into a smaller operation, a delayed operation, or a plan without surgery.
The 4 slides below split this section into one practical point per image. Swipe sideways, use the arrows to move one slide at a time, or use the numbered controls under the image to jump to a specific slide.
Details to bring to the consultation
Bring clear information, not just a fear that baldness runs in the family. Useful details include the age when close relatives started losing hair, their current pattern, whether the crown became involved, whether the sides and nape stayed strong, whether anyone used medication, and whether anyone had a transplant. Old photos can help if they show the age and pattern clearly.
For your own hair, bring dated photos in the same lighting when possible. Include front, temples, mid scalp, crown, donor, and wet hair views if density is the concern. Add the approximate date, age, medication status, and whether the hair was wet, styled, colored, or cut shorter than usual. If you already have a proposed graft count from another clinic, bring it. The family pattern may explain why a large graft count looks tempting, but the donor exam decides whether it is wise.
The consultation should end with a donor budget, not only a hairline sketch. You need to know what is being treated now, what is deliberately being left for later, what family history clues made the plan more conservative, and what warning signs would change the plan before surgery.
Family history is more useful when the consultation includes dates, photos, and treatment details, not only the statement that baldness runs in the family.
Second opinion timing
A second opinion is worth getting when the proposed plan ignores strong family history, promises a very low hairline in a young person, spends heavily on the crown early, or gives a graft count without examining donor quality. It is also useful when several relatives reached advanced baldness and the current proposal has no reserve strategy.
Possible advanced patterns should be compared with Norwood 6 to 7 hair transplant planning, not judged like a routine hairline case. For mild early recession, Norwood 2 hair transplant planning carries a different safety margin. The same number of grafts can be reasonable in one person and unsafe in another because the future demand is different.
If the answer you receive is only “you need 4,000 grafts” without a discussion of age, family pattern, miniaturization, donor reserve, and medication suitability, the plan is incomplete. A surgical plan has to fit both today’s mirror and the pattern you may still develop.
Surgery should still fit the family pattern
Desire and sequence are not the same. You may want a lower hairline now, but stabilization, observation, or a smaller frontal design may need to come first. You may want the crown filled, but the graft budget may need to protect the mid scalp first. The family pattern helps set the sequence.
I become more comfortable when the current loss is measurable, the donor is strong enough, the hairline is age appropriate, the crown request is realistic, and you understand that continued hair loss after a hair transplant can still change the native hair around the grafts.
Baldness in the family is only the starting point. I need the first operation to still look responsible if your family pattern appears more strongly later. Strong family baldness does not have to block surgery, but it raises the standard for proof that the design will age well. It requires a plan that spends grafts as if the future still matters.