



Surgeon Involvement in Hair Transplant Surgery
Before you commit to a hair transplant, you should know exactly who will examine the donor area, design the hairline, give or supervise anesthesia, create extraction or recipient area incisions, control graft handling, and review the final plan. When those roles are vague, the operation is already harder to trust before it begins. The same standard applies when a clinic promotes robotic hair transplant technology, because the device does not name the person responsible for those decisions. That clarity becomes even more important when a patient arrives with AI hair transplant planning notes that sound confident but have not examined the scalp.
A trained team can be part of a well planned operation. The concern is not teamwork. The concern is when the advertised surgeon becomes only a name on the website while the decisive medical and aesthetic steps are handled through an unclear high volume system. You may only discover the difference after the hairline, donor area, or graft direction has already been changed permanently.
If you are comparing clinics, use this page to judge what surgeon involvement should mean in a real hair transplant, not only in marketing language.

My plan review before surgery
Before I accept a case, I do not start with the package or the promised graft number. I first look at whether the donor supply can support the result, whether the hairline can age naturally, and whether the recipient area belongs in one stage or a slower plan.
That means I may reduce the graft number, change the hairline, delay crown work, or say no when the plan would spend too much donor hair for a result that will not hold. Surgeon involvement should be visible in these decisions, not only in a signature, a short greeting, or a clinic name on the website.
Responsibility belongs before surgery
The strongest booking decision is made before payment, travel, or emotional commitment. You should be able to ask a basic process question and receive a specific answer. You should know who will design the hairline, who will perform the surgical incisions or extraction work, who will supervise graft preparation, who will place grafts, and who will be medically responsible if something changes during surgery. Ask for that answer in writing before the deposit, not only in a quick sales call, because hair transplant booking pressure can make unclear roles feel acceptable too early. This is also where how many hair transplant patients are booked in one day matters, because surgeon involvement needs enough time to be real.
Clinic fame or a large graft package does not answer the surgical responsibility question. It also should not be enough to accept a best hair transplant clinic in Turkey claim without seeing where the surgeon’s judgment enters the plan. If you are still comparing clinics, the broader guide on before surgery booking clarity can help, but surgeon involvement deserves its own decision because it affects every technical step after the date is set.
The answer does not need to sound dramatic. It needs names, roles, limits, and consistency. If the clinic will not explain who controls each step, you are being asked to trust a system that has not been made visible.
Judging real surgeon involvement
For me, surgeon involvement is not a sentence on a website. It is whether I can show where my judgment enters the plan, the hairline design, the surgery day decisions, and the follow up after the patient goes home. Use the 10 surgeon involvement proof slides below to separate before booking review, donor reserve, hairline design, anesthesia responsibility, extraction limits, recipient angles, graft handling, team roles, day of changes, and aftercare context. Swipe sideways, use the arrows, or choose a number below the image.
If a patient cannot place the surgeon in that pathway before booking, the claim of surgeon involvement is too abstract to guide a serious decision.
A surgical team is normal when responsibility stays clear
Hair transplantation usually involves more than one pair of hands. Graft counting, graft sorting, graft hydration, room preparation, patient monitoring, and instrument handling can involve trained staff. In a well run operation, the team supports the plan.
The distinction is who carries medical responsibility. A team can assist inside a controlled system, but the diagnosis, hairline design, donor management, anesthesia safety, extraction pattern, recipient area strategy, and response to medical issues cannot be left to a sales office or an unnamed system. They require medical judgment and a clearly named doctor responsible for you, not only for the schedule.
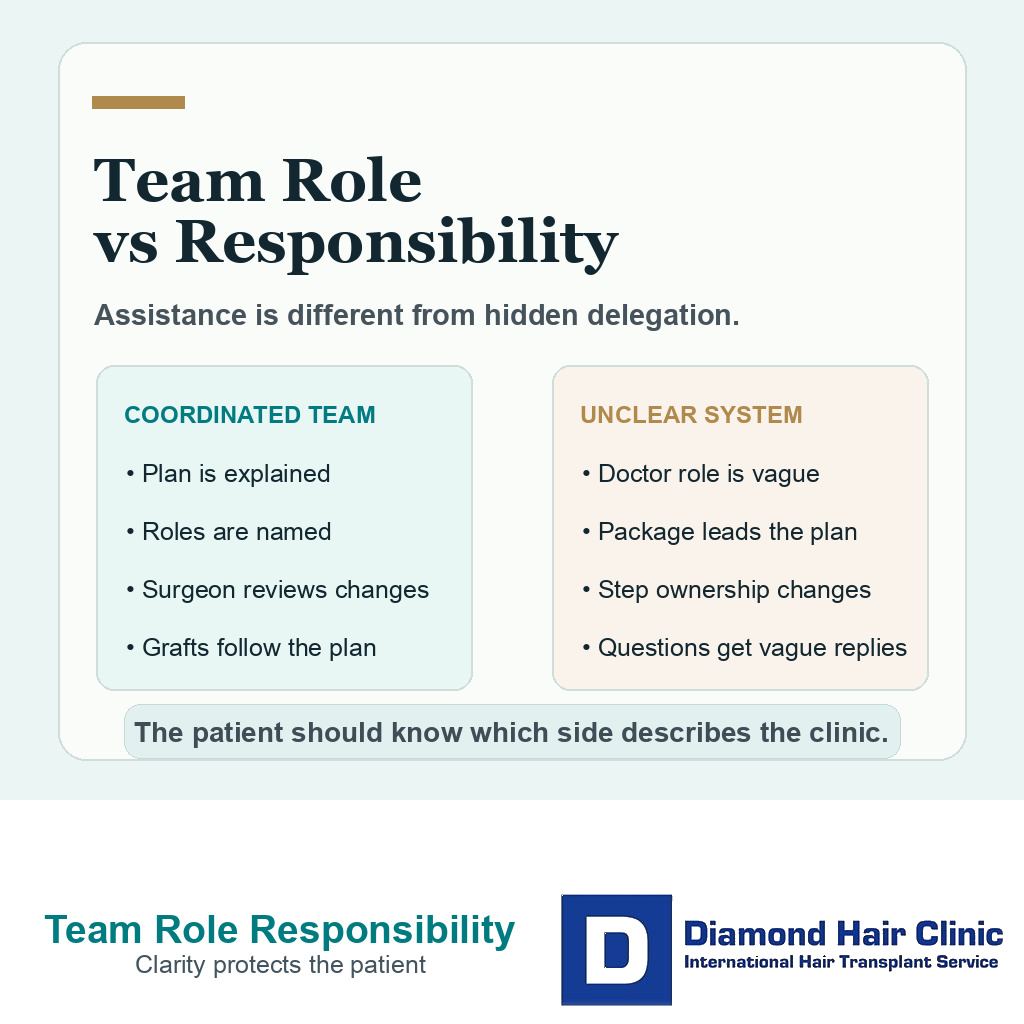
When a clinic says “our team does the procedure,” ask what that sentence actually means. In one clinic, it may describe trained assistants working under a clear surgical plan. In another, it may hide the fact that the surgeon’s role is brief, unclear, or mostly symbolic. Also ask whether the surgeon is responsible for more than one operating room or patient at the same time, because physical availability matters when the plan needs adjustment.
Hairline design belongs with medical planning
Hairline design, like a visible mustache transplant design, is not drawing a nice line on the forehead. It is a medical and aesthetic decision tied to age, facial proportions, donor capacity, future hair loss, hair caliber, curl, skin contrast, graft supply, and the possibility of needing another procedure later.
Hairline design should not be separated from the surgeon’s examination. A low or dense hairline can look attractive in a consultation photo and still be unsafe for your long term pattern. A straight line can look clean on a marker drawing and later look artificial once the transplanted hair grows.
The person designing the hairline needs to understand how the donor area will pay for that design. The same person should be willing to say no when the requested line is too low, too dense, too straight, or too expensive in grafts for the future. A hairline that cannot age with you is not a successful design.
Responsibility for extraction and recipient openings
FUE extraction is not only removing hair from the back of the head. Every punch changes the donor area. The pattern, spacing, depth, angle, and total number of extractions affect whether the donor looks even, whether short haircuts remain possible, and whether there is enough donor supply for future loss.
The same applies to openings made in the recipient area. The angle, direction, density, and distribution of tiny openings determine whether the hairline blends naturally or looks pluggy, upright, sparse, or crowded. Graft number planning matters, but the number alone does not protect the donor area if the extraction pattern is careless.
Before surgery, the clinic should be able to explain who makes these decisions and who performs the steps that create incisions or excisions. Laws and delegation rules differ by country, but your practical question stays the same. You need to know who is medically trained, named, present, and accountable for the parts of the operation that alter living tissue. If a step is delegated, the clinic should say exactly which step, to whom, and under what direct control.
Do not accept an impressive graft number as a substitute for named surgical responsibility. Overharvesting can be very difficult to repair. With donor area overharvesting, donor preservation has to be protected before the first punch is made.
Graft handling needs controlled roles
Graft handling is a team step where control matters. Follicular units must be kept hydrated, organized, protected from unnecessary trauma, and placed according to the plan. A skilled assistant can matter here, but only inside a system where the surgeon has already decided the distribution and is available to correct the plan if the graft count, graft quality, bleeding, or recipient area changes.
People often focus on the method name, such as Sapphire FUE, DHI, micro motor, implanter pen, robotic assistance, or another branded tool. Hair transplant tools and techniques have limits. A tool does not decide whether a single hair graft belongs in the first row, whether a multi hair graft will look coarse at the hairline, or whether the crown should receive fewer grafts to protect the front.
If graft placement is delegated, the clinic should still be able to show how direction, density, row softness, and graft selection are controlled. A vague answer about “experienced” technicians is not enough if no one describes how the surgeon’s plan becomes the final placement pattern.
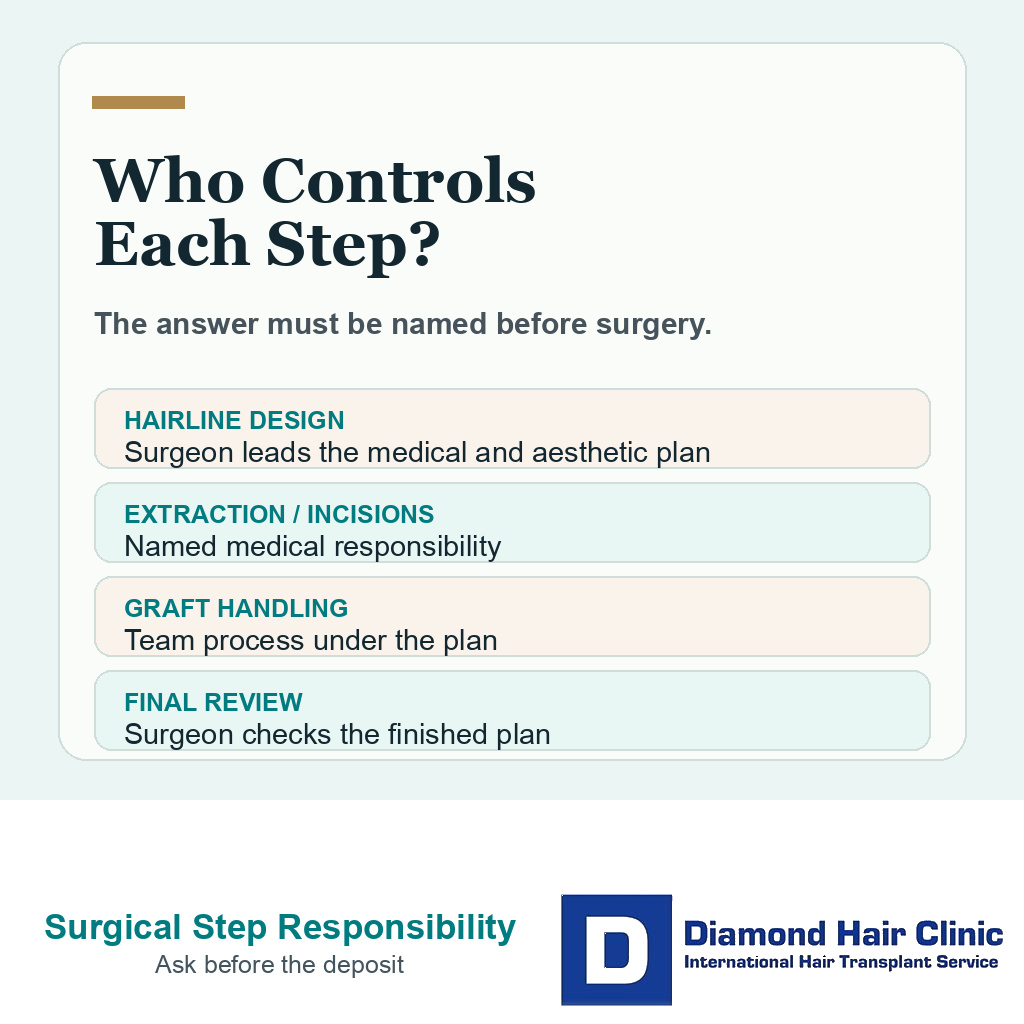
Surgeon involvement has to be visible in diagnosis, hairline design, incision or extraction responsibility, graft strategy, and final review.
Anesthesia and medical reactions are not sales details
Local anesthesia makes hair transplant surgery more comfortable, but it is still medication entering your body. Dose, medical history, blood pressure, anxiety, heart disease, allergies, and drug interactions all need attention. Pain control matters, but medical responsibility matters more if the body reacts unexpectedly.
A high volume schedule can make the procedure feel routine. That routine feeling should not replace medical review. Surgery can be routine for the clinic and still medically personal for the person sitting in the chair. If the medical review is rushed, the surgical day becomes weaker before graft work even begins.
A controlled schedule, direct surgeon review, and time to notice medical details matter here. A rushed room can miss information that a more deliberate medical process would catch.
A specific consultation answer should name roles
A useful consultation answer gives names, roles, and limits. It tells you who will design the hairline, who will evaluate the donor area, who will be in the operating room, who performs or directly controls surgical incisions or extraction, who handles graft sorting and placement, and who reviews the result before you leave. It should also explain the checkpoints. Those include donor review after shaving, final hairline confirmation before anesthesia or incisions, and who checks the graft distribution before implantation continues.
Weak answers sound polished but incomplete. “Our team is experienced,” “the doctor supervises,” “everyone is certified,” or “we do thousands of cases” may be true in some clinics and still not answer the real question. You need to know what happens during your own operation.
The word “supervises” also needs detail. It can mean the surgeon is physically present, checking the plan and able to intervene. It can also mean the surgeon is only named in the background while other people run the operation. Those are not the same level of responsibility.
When a clinic can answer clearly, the conversation becomes easier to judge. You can then compare skill, planning, recovery, cost, and aftercare with more confidence. If the answer changes from one message to another, treat that inconsistency as a reason to slow down.
A changed surgeon role on procedure day
If the named surgeon, the promised role, or the surgical team changes on the day of the procedure, do not treat it as a small scheduling detail. Ask again who will examine the donor area, confirm the hairline, give or supervise anesthesia, perform extraction or recipient area openings, and stay responsible if the plan changes during surgery. Pause before shaving, anesthesia, or incisions if the explanation no longer matches what you accepted.

A change is not unsafe by itself, but it must be explained before irreversible steps begin. You need to meet the doctor who is actually responsible, understand what that doctor will do, and feel free to delay if the explanation is different from what was promised before the trip. Consent is weaker when you learn the real surgical arrangement only after travel, shaving, sedation, or payment pressure. Consent is also weaker when language barriers during a hair transplant abroad prevent the patient from understanding who performs the key steps.
High volume warning signs before a deposit
Not every busy clinic is unsafe, and not every small clinic is excellent. Volume by itself is not the full answer. The warning signs appear when you cannot identify the surgeon, cannot learn who performs each surgical step, cannot get a direct medical review, or are pushed toward a date, discount, or package before the plan is clear. Another warning sign is when before and after examples are shown without confirming whether the same surgeon and team structure will be involved in your operation.
When you look at before and after photos and hair transplant reviews, ask whether those examples reflect the same surgeon, same team, same hair type, same donor quality, same loss pattern, and same clinic structure. Photos can show an outcome, but they do not always show the case reasoning behind it.
Low price can also distract from responsibility. A cheap hair transplant abroad can become expensive when repair work, depleted donor supply, or poor follow up enters the picture.
Repair cases are harder than first surgery
A weak first surgery can leave more than disappointment. It can leave a low hairline that is hard to redesign, wrong graft direction, multi hair grafts in the front row, depleted donor supply, visible extraction thinning, scarring, or a result that looks acceptable in one photo but fails in real lighting.
Repair is possible in selected cases, but it is often slower, more expensive, and more limited by donor supply than planning the first surgery correctly. In some cases, bad hair transplant repair may require camouflage, removal, redistribution, a second session, or accepting that some damage cannot be fully erased.
Pluggy hairline cases show this clearly. In certain cases, pluggy hairline repair can improve softness, but it must work with the grafts and donor supply that remain. Surgeon involvement before the first surgery protects those options.
The cheapest unclear operation can become the most expensive decision if grafts are spent badly.
Method names do not replace responsibility
Technique names can help describe an operation, but they do not prove the operation is well planned. Sapphire FUE, DHI, robotic support, implanter pens, or any other device can be used well or poorly. The decisive issue is the plan behind the device.
A clinic may advertise a modern tool and still use an aggressive hairline, weak donor selection, unclear surgeon presence, or poor graft direction control. Another clinic may use a familiar method with excellent planning and careful execution. Compare medical responsibility before comparing method names.
This is especially relevant when a clinic promises very high graft counts, dramatic density, or a full transformation in one day. The stronger question is how the surgeon will protect the donor area, future hair loss, natural direction, and follow up if your scalp does not match the advertisement.
A trained team can support hair transplant surgery, but unclear responsibility should not be hidden behind the word team.
Follow-up is part of surgeon involvement
Surgeon involvement does not end when the patient leaves the operating room. Early swelling, donor discomfort, crusting, shedding, uneven growth anxiety, and photos sent from another country all need to be read against the plan that was actually performed.
When I review follow-up photos, I am not judging a random scalp image. I compare the concern with the donor map, graft distribution, hairline design, crown decision, medical history, and the stage of healing. That context is what separates useful guidance from generic reassurance.
This is also why result photos should not be interpreted away from responsibility. A clinic that shows strong before and after images still needs to explain who reads early recovery photos, who decides when local care is needed, and who understands the surgical choices behind the result.
Judging the clinic response
The clinic’s answer should leave you with a clear mental picture of the surgical day. The surgeon reviews the donor and recipient areas, the hairline plan is medically and aesthetically explained, the graft number is tied to donor capacity, the roles inside the room are named, and you know who is responsible if the plan changes. You should also know who reviews your early photos, donor area concerns, infection questions, or unexpected symptoms after you leave the clinic.
For me, surgeon led planning in Istanbul means the surgical plan stays connected to medical responsibility. You are not treated as a package moving through a room. The donor area, hairline, graft distribution, and follow up all belong to the same long term plan.
Waiting for the right doctor can be better than accepting an earlier date with weaker clarity. Waiting for the right hair transplant surgeon can feel frustrating for a few extra weeks or months, but repair surgery after an unclear first operation can take years to manage.
The final decision should be practical, even when the emotion around it is not. If the clinic can explain who controls the medical and aesthetic steps, you can judge the plan. If the answer remains vague, you are not only choosing a clinic. You are accepting uncertainty inside the operation itself.
Surgeon role clarity also belongs in the booking messages. The booking messages and surgical plan check focuses on matching the official channel, role map, and planned surgical steps before commitment.