Thyroid Stability and Surgery Timing
A hair transplant may be possible if you have thyroid problems, but I do not plan surgery until the thyroid condition is diagnosed, treated, and reasonably stable. If thyroid levels are actively changing, medication was recently adjusted, symptoms are strong, or shedding is sudden and diffuse, I usually wait before using donor grafts. The same diagnosis first timing matters for women considering a hair transplant with PCOS, where hormones and shedding can blur the surgical picture.
This matters in a very practical way. A hair transplant moves healthy donor follicles into areas of permanent thinning. It does not correct hypothyroidism, hyperthyroidism, Hashimoto’s thyroiditis, Graves’ disease, or any other thyroid imbalance. If the thyroid problem is still disturbing the hair cycle, the operation may be technically correct, but the patient may still feel that the result is confusing because native hair keeps shedding around the transplanted grafts.
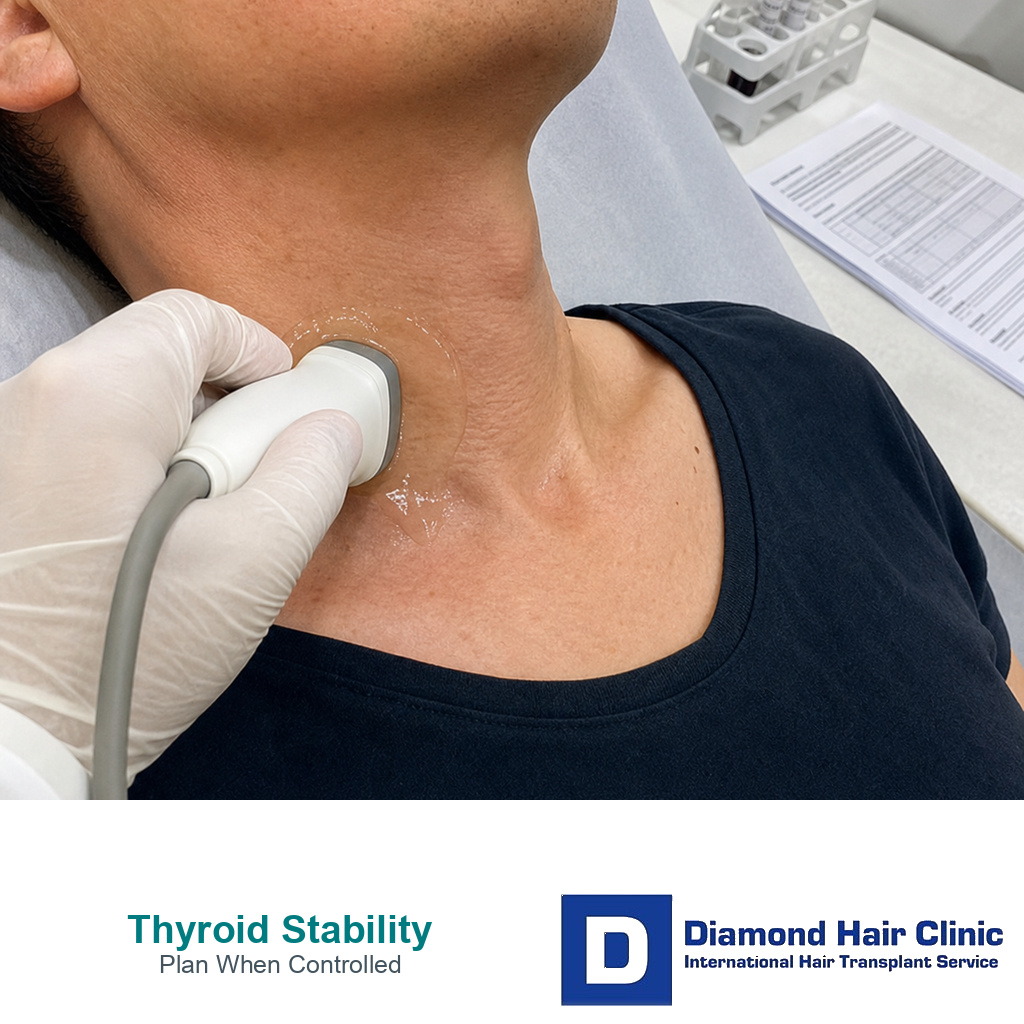
The diagnosis label alone is not enough to accept or reject surgery. I need to know how controlled the thyroid condition is right now. Stable does not mean perfect forever. It means the recent blood results, medication dose, symptoms, and shedding pattern are not moving in a way that would mislead the surgical plan. Hair transplant timing with thyroid disease depends on both medical control and a readable hair pattern, not one lab result. When the thyroid picture is not stable, the safer first step is medical control and observation.
Thyroid levels matter before a hair transplant
Thyroid hormones influence the hair cycle. When the thyroid is underactive or overactive, some patients develop diffuse shedding, reduced hair quality, dry or brittle hair, eyebrow thinning, or a general loss of volume that does not behave like simple pattern hair loss.
It matters because hair transplant planning depends on reading the scalp correctly. I need a clear picture of which hairs are permanently miniaturizing, which hairs may recover after medical treatment, and which areas truly need grafts. If those questions are blurred by active thyroid imbalance, the plan can become too aggressive or simply poorly timed.
The same diagnosis first logic applies to other medical causes of shedding. A hair transplant after cancer treatment, or a case with abnormal blood tests before a hair transplant, should not be planned from one photograph while the medical background is still unclear.
Thyroid disease can look like balding
It can. Thyroid related shedding can make the scalp look thinner even when the underlying pattern hair loss is not severe. Some patients notice hair falling from all over the scalp. Some notice weaker hair texture. Some feel that their hair suddenly lost body and coverage.
That can look frightening, especially for a patient who already has male pattern hair loss. The difficult part is that both problems can exist together. A patient may have real hairline recession and crown thinning, and still have thyroid related diffuse shedding at the same time.
If I transplant without separating these problems, the surgery may answer only one part of the patient’s concern. The grafts may grow, but the patient may still feel thin because the surrounding native hair is going through a medical shedding phase. Diagnosis has to come before design.
Separating thyroid shedding from pattern hair loss
Pattern hair loss usually follows a recognizable map. The hairline recedes, the temples weaken, the crown opens, or the mid scalp gradually loses density in a predictable way. Thyroid shedding is often more diffuse. It may affect the whole scalp, and the timing may be sudden or connected with symptoms, medication changes, illness, weight change, or abnormal blood results.
In consultation, I look at the donor area, the miniaturization pattern, the family history, the speed of change, and the medical history. I ask when shedding started and whether it changed after thyroid treatment. A patient with diffuse thinning should not be planned in the same way as a patient with a stable frontal recession.
Sometimes the answer is not available in one visit. A few months of stable thyroid treatment and consistent photographs can make the picture much clearer. Waiting is not a weak decision when the diagnosis is still moving. It can protect the donor area and prevent a design based on temporary thinning.
If I would delay surgery
I delay surgery if the thyroid diagnosis is new, the medication dose was recently changed, the blood results are clearly abnormal, or the patient has strong symptoms such as unexplained weight change, fatigue, tremor, heat intolerance, cold intolerance, racing heart, or marked anxiety connected with thyroid imbalance.
I also wait if shedding is sudden and heavy. If hair is falling from the entire scalp, the first question is not where to place grafts. The first question is why the hair cycle is disturbed. Surgery should not be used to cover uncertainty.
Waiting does not mean the patient can never have surgery. It means the thyroid condition should be controlled enough for the hair loss pattern to be judged fairly. A delayed operation can be a better operation if it gives the surgeon and the patient a clearer map.
Thyroid medication usually does not prevent surgery
Usually, no. Thyroid medication by itself is not a reason to reject a patient. Many patients who take thyroid medication can still be candidates for surgery when the condition is stable, the treating physician is satisfied, and the hair loss pattern is suitable for transplantation.
What I avoid is sudden medication change made only because of surgery fear. Do not stop thyroid medication before a hair transplant unless the treating physician specifically advises it. Stability is usually more helpful than panic.
If the patient recently started medication, recently changed the dose, or still has symptoms, I need a period of stability before final surgical planning. The issue is not the word thyroid. The issue is whether the body is in a steady enough state for the plan to be reliable.
Starting thyroid treatment is different from being stable on thyroid treatment. I do not need perfection, but the dose, symptoms, and shedding pattern should stop changing in a way that would mislead the plan. Otherwise, the transplant may be judged while the scalp is still reacting to a medical problem.
This 10 slide carousel explains why thyroid stability comes before judging shedding or surgery timing. Swipe sideways, use an arrow, or choose a number below the image.