Microneedling Timing Before FUE Surgery
Before surgery, I worry less about the microneedling habit itself and more about whether the scalp is quiet enough to accept incisions. Light, shallow microneedling should usually stop at least 2 weeks before surgery if the scalp has settled. Deeper sessions, frequent treatments, visible bleeding, professional treatments, or anything irritating should stop at least 4 weeks before surgery, and sometimes longer if the scalp is still red, tender, flaky, or inflamed.
I avoid creating recipient area incisions through skin that is already irritated. A hair transplant needs settled skin, stable blood supply, clean healing, and controlled incision angles. If the scalp looks settled by the time I examine it, previous microneedling may not change the plan very much. If the scalp is reactive, delaying the operation is safer than gambling with donor grafts.
I separate two situations. One light session that stopped early enough and left the skin quiet is different from repeated deep needling, bleeding, scabbing, or strong products used close to surgery. No pain does not always mean the skin is ready.
Microneedling before surgery is not always a problem
In most cases, no, if it was done sensibly and stopped early enough. Many patients have used microneedling as part of a hair loss routine before they ever think seriously about surgery. That history alone does not make someone a poor candidate.
The concern begins when microneedling is done too close to the operation, too deeply, too often, or on a scalp that reacts badly. Being a good candidate for a hair transplant is not only about age, donor density, and hair loss pattern. It is also about whether the scalp is healthy enough to heal predictably.
A hair transplant is performed through real tissue. If that tissue is settled, I can plan more accurately. If it is inflamed, crusted, or unpredictable, the safer plan may be to wait.

The scalp needs a break before surgery
Microneedling should stop before surgery because it creates controlled injury. That is the purpose of the treatment. The skin responds with inflammation, repair, and sometimes redness or sensitivity. This is acceptable in the right treatment window, but not ideal just before I need to make a precise surgical plan.
During hair transplant surgery, I create thousands of precise recipient area incisions. Around the frontal hairline, the angle and spacing of those incisions matter. Hairline design is not only a drawing. It depends on skin quality, direction, density, and how the grafts will sit after healing.
When the scalp is already healing from repeated needle trauma, the operation adds surgical injury to skin that may still be in a repair phase. That is not the right environment for a planned operation.
Stop timing depends on depth and healing
For light home microneedling with shallow needles and no irritation, I usually want at least 2 weeks without needling before surgery. That gives the scalp time to settle and gives me a clearer picture of the skin.
For deeper needling, frequent sessions, visible bleeding, professional treatments, or any strong reaction, I usually want at least 4 weeks and sometimes longer. If the scalp still looks red, tender, oily, crusted, thickened, or irritated, the calendar does not matter. The skin is not ready.
The skin tells me more than the date. Moving the operation is better than spending the day trying to place grafts into tissue that is not behaving normally.
Needle depth and bleeding change the risk
Needle depth matters because shallow stimulation and deeper trauma are not the same thing. A short, gentle session that causes only mild temporary pinkness is different from repeated deep needling that causes bleeding, prolonged redness, or scabbing.
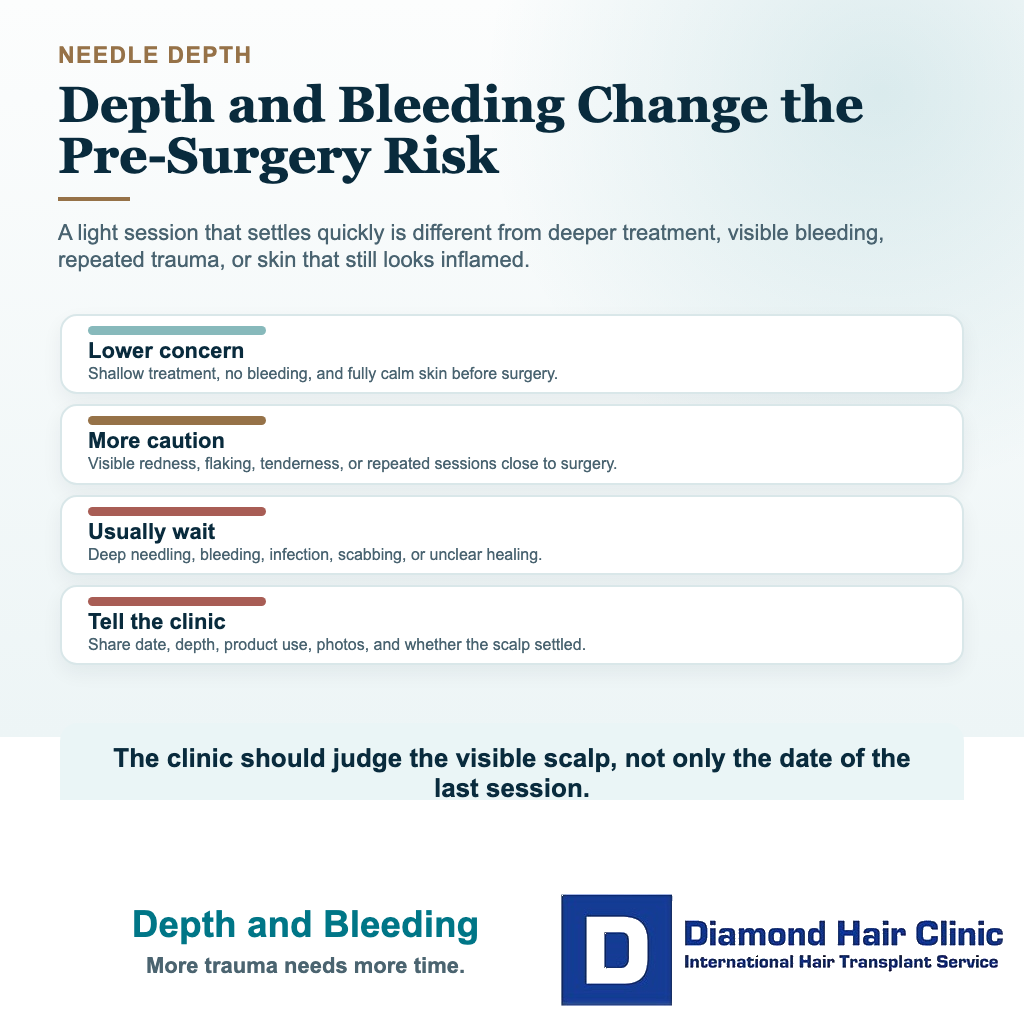
Bleeding itself is not proof that microneedling is effective. Some patients believe more bleeding means more benefit. In surgery, I do not think that way. Controlled injury and uncontrolled irritation are different clinical situations.
If a patient has been using long needles, pressing hard, or combining needling with strong topical products, that history should be clear before surgery. This is not about blame. The goal is to protect the grafts and choose the safest timing.
Scar tissue risk in the recipient area
Light, sensible microneedling usually does not create scar tissue that makes a transplant impossible. But aggressive needling, repeated inflammation, infection, or poor technique can change the skin. The issue may not be an obvious scar. It may be subtle firmness, uneven texture, persistent redness, or skin that does not accept incisions smoothly.
In the recipient area, incision spacing and density need careful judgment. If the skin is fibrotic or reactive, I may need to reduce density, spread the work more conservatively, or delay the case. Too many grafts in one area is already a risk when tissue limits are ignored. Irritated tissue makes that discussion more serious.
A transplant plan should not force density into skin that is asking for caution.
Scalp signs that can delay the operation
I delay surgery if I see redness that does not settle, tenderness, pustules, crusting, open scratches, active flaking, shiny thickened skin, or signs of infection. These signs tell me that the scalp is not settled enough for elective surgery.
This matters after surgery too. A patient with an already irritated scalp may panic when normal early redness, scabs, or small bumps appear. Redness, scabs, and pimples after a hair transplant need context before the patient assumes something is wrong.
Starting from settled skin makes early recovery easier to interpret. That helps both the surgeon and the patient.
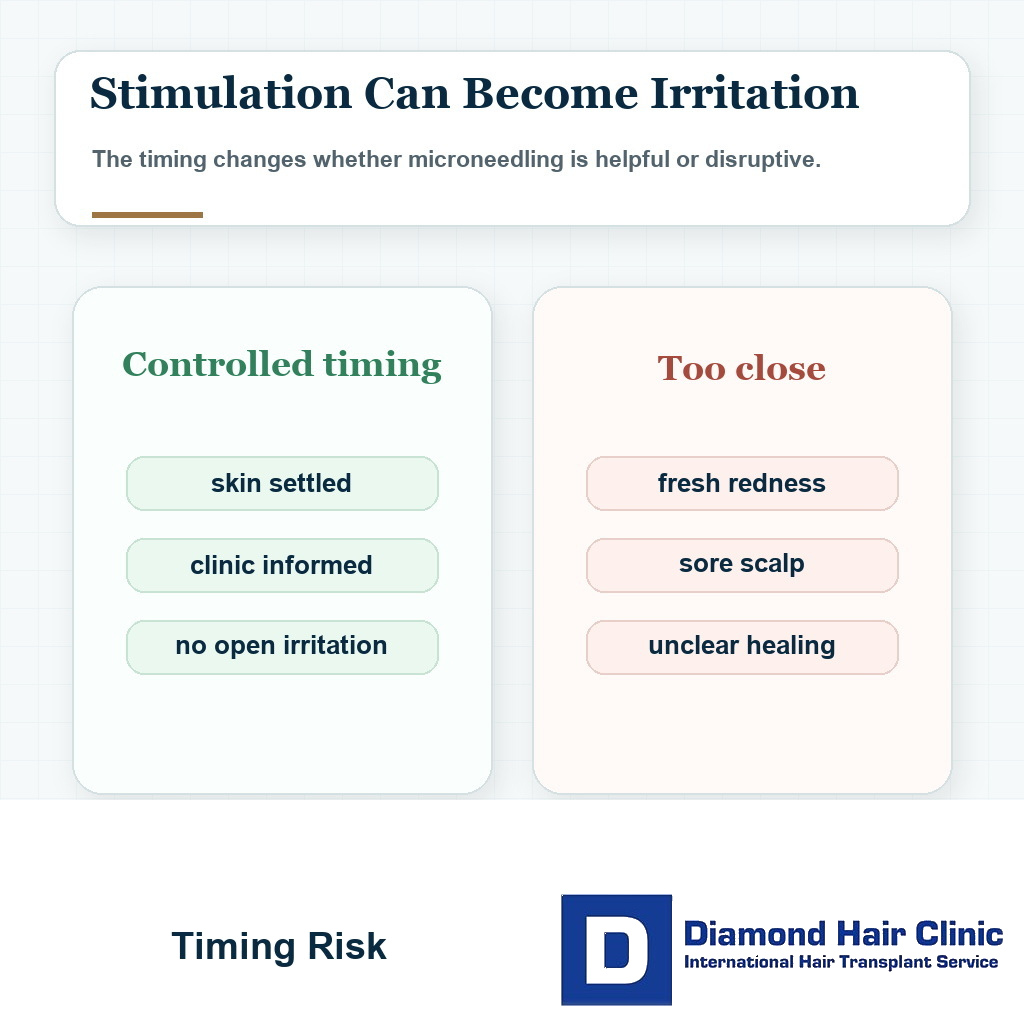
Microneedling readiness filter
Is the scalp ready after microneedling?
Use this before one last needling session turns into a surgery day skin problem.
If the scalp is closed, calm, and easy to examine, surgery may still be reasonable. If the timing is shorter or the skin is reactive, the plan needs surgeon review.
Minoxidil and other products change the timing
The product used after needling matters. Many patients microneedle and then apply topical minoxidil, oils, acids, serums, or mixed products. Sometimes the irritation comes less from the needle and more from what was applied afterward.
Needling should not be used as a way to force every product deeper into the skin, especially in the weeks before surgery. A topical that is harmless on intact skin can feel very different after small needle channels have been created.
If a topical product burns, flakes, dries the scalp, or causes redness, the reaction should settle before surgery. Stopping minoxidil before a hair transplant is partly about timing and partly about scalp irritation. Adding it immediately after needling may make the scalp more reactive in some patients.
Medical treatment can be useful when it is appropriate. The difficulty is last minute irritation. The final weeks before surgery should let the scalp become predictable, not challenge it again.
Microneedling may help hair before transplant planning
Microneedling may have a place in some nonsurgical hair loss routines, especially when it is used thoughtfully with medical treatment. But a treatment can be useful at one stage and unwise at another stage.
Before surgery, the priorities change. I am thinking about the healing environment for the grafts, incision control, infection risk, bleeding, and whether the recipient area is stable. Medication before a hair transplant needs planning in advance rather than mixed with aggressive scalp stimulation in the final days.
If microneedling has helped the patient feel proactive, I understand that. But once surgery is scheduled, doing less for a short period often protects the operation better than doing one more session.
Microneedling does not set the graft number
Normal scalp findings mean microneedling may not change the graft number. If the recipient area is irritated, thickened, or unpredictable, it can change the plan. I may reduce density, split the work, or delay until I can reassess.
Graft numbers differ between clinics because responsible planning should consider donor capacity, hair caliber, recipient area size, skin condition, and long term goals. A graft number should not be treated like a fixed shopping number.
The recipient area is not empty space. It is living tissue that must accept and heal around the grafts.
Donor area microneedling needs separate review
Most patients think only about the recipient area, but the donor area also matters. If the back or sides of the scalp were microneedled recently, I check whether there is tenderness, redness, folliculitis, or surface irritation there too.
FUE extraction depends on clean donor skin and predictable graft release. If the donor area is inflamed, the extraction can become less comfortable and less predictable. The donor area also has to heal after thousands of small extraction points, so I avoid it irritated before we start.
Donor microneedling does not always cancel surgery. It means the donor skin needs judgment with the same seriousness as the recipient area. The plan needs to protect both sides of the operation.
The 9 microneedling timing slides below separate last session timing, needle depth, recipient skin, texture changes, red flags, product irritation, donor area review, one week disclosure, and restart logic after surgery. Swipe sideways, use the arrows one slide at a time, or choose a number below the image.