


Low White Blood Cells and Hair Transplant Timing
A hair transplant can sometimes still be possible with low white blood cells, but I need to know which white cell is low and why. The total WBC number is only the first clue. A low neutrophil count, especially with fever, recent infection, mouth ulcers, skin infection, medicine that affects the immune system, or no medical clearance, can make surgery wait. For the same reason, a cold or flu before hair transplant surgery should be reported rather than hidden.
If your neutrophils are clearly low, the safer answer is often to repeat the blood test, understand the cause, and delay travel until the clinic can review the result properly. Hair transplant surgery is elective. Protecting the scalp, donor area, and general health comes before keeping a convenient date.
A mild, explained result that has been present for a long time is a different surgical conversation from a new, falling, moderate, or severe neutrophil result, especially with fever, mouth ulcers, skin infection, recent antibiotics, or medicine that affects the immune system.
infection readiness map
Which low WBC finding changes surgery timing?
Choose the part of the blood result or symptom picture that matches your case. The decision changes when the neutrophil count, infection signs, medicine history, or wider CBC pattern changes.
A stable mild result may still be workable
I still need the full CBC with differential, older results, infection history, and any doctor note. Surgery may stay possible when the pattern is long standing, explained, and not linked with recurrent infections.
The ANC changes the surgical question
The total WBC number is not enough. If the absolute neutrophil count is clearly low, the case needs repeat testing, cause review, and medical clearance before elective scalp surgery is planned.
Symptoms move the decision away from surgery
Fever, chills, mouth sores, painful urination, draining wounds, cough, or skin infection need medical review first. A hair transplant date should wait when infection defense is unclear.
A recent illness can make the count temporary
COVID, flu, dental infection, antibiotics, or recent recovery can affect the result. The useful next step is often a repeat CBC after symptoms settle, with timing explained before travel is arranged.
Medicine history must be coordinated
Do not stop immune or monitored medicine on your own. Send medicine names, dose, start date, last dose change, and the prescribing doctor’s advice before the surgical plan is treated as final.
Several abnormal results lower the threshold to wait
Low neutrophils with low hemoglobin, low platelets, abnormal flags, liver or kidney issues, or unclear diagnosis is not a small administrative problem. I want a medical explanation before surgery is arranged.
This map does not clear surgery. It shows why I ask for the full differential, symptoms, medicine history, and medical context before travel is treated as safe.
Low WBC or low neutrophils can delay surgery
Low white blood cells can delay a hair transplant when the result suggests that your body may not control infection predictably. The concern becomes stronger if the abnormal result is new, unexplained, repeated, or linked with fever, recent illness, mouth ulcers, skin infection, swollen glands, unusual fatigue, or medicines that affect the immune system.
In hair transplant surgery, the donor and recipient areas are opened through many small channels. The procedure is usually safe when you are medically ready, but it still depends on clean healing. If the white cell result suggests reduced infection defense, proceeding without review can turn a preventable delay into a larger problem.
A broad blood test before a hair transplant helps the clinic see this before the surgical day. The value of the test is not only finding a problem. It also protects you from travelling, shaving, starting anesthesia, and then being told that the procedure must stop.
A single low result does not always mean surgery is impossible. It means the result needs context. Was the test taken after COVID infection or another recent virus? Has the count been low for years without infections? Did a medicine change recently? Are neutrophils low, or is only one lymphocyte line slightly below the lab range? These details decide whether surgery can continue, wait briefly, or needs specialist review.
Neutrophils matter more than the total WBC number
The total WBC number is only the headline. The differential count shows which white cell type is low. For surgery, neutrophils deserve special attention because they are a major defense against bacterial infection. When neutrophils are low, the medical word is neutropenia, and the number I need to see clearly is the absolute neutrophil count, often written as ANC.
Do not rely on percentages alone. If the report shows neutrophils as a percentage but not the absolute neutrophil count, send the full differential or ask the laboratory for the absolute value. Reports may write this as ANC, absolute neutrophils, neutrophils absolute, GRAN absolute, or x 109/L. The unit matters because a percentage cannot tell the surgical risk by itself.
Many hematology references describe neutropenia as an absolute neutrophil count below about 1.5 x 109/L. Mild neutropenia is often around 1.0 to 1.5. Moderate neutropenia is around 0.5 to 1.0. Severe neutropenia is below 0.5. These ranges are not hair transplant permission rules, but they help explain why a clinic becomes more careful as the neutrophil count falls.
WBC 3.0 with neutrophils 0.87 x 109/L is not the same as a mildly low total WBC with a stable neutrophil count. The second situation may be less concerning if it is chronic and explained. The first often deserves delay, repeat testing, and medical review before an elective procedure.
The surgical concern is also local. If there is active scalp inflammation, folliculitis, open irritation, or infection, a low neutrophil count becomes more relevant. My threshold for comfort is different when the scalp is clean and stable compared with a scalp that already shows pustules, crusting, or inflamed skin. If infection appears after surgery, the warning signs of an infected hair transplant need quick contact with the clinic.
One low white blood cell line needs context
I ask for the full CBC with differential, not only the total WBC number. A slightly low total WBC with a stable neutrophil count is not the same as a clearly low absolute neutrophil count. A low lymphocyte count, an isolated mild change after a recent virus, or a chronic result your doctor already knows may lead to a different decision from a new neutrophil drop.
The trend also matters. A single result just below the lab range may only need a repeat test. A falling count, several abnormal blood lines together, or low WBC combined with low hemoglobin or low platelets needs more caution. If the report includes abnormal flags or comments, send the full page rather than cropping the result to the WBC line.
For surgery, I am not looking for a perfect laboratory report. I am looking for a pattern that is medically explained and stable enough for elective scalp surgery. If the differential count is unclear, the safest next step is repeat testing or a short note from the doctor who knows your blood history.
Mildly low count may still be acceptable
Sometimes, yes. A mildly low white cell count can be acceptable when it is stable, already known, not linked with recurrent infections, and your doctor has explained the reason. Some people naturally run lower than the printed range. I do not cancel surgery only because one number is slightly outside the laboratory reference range.
The decision changes when the count is dropping, the neutrophil count is moderate or severe, the result is new, or there are other abnormal results in the same CBC. Low hemoglobin, low platelets, abnormal liver or kidney results, or inflammation markers can change the whole picture. I need the full report, not only a screenshot of the WBC line.
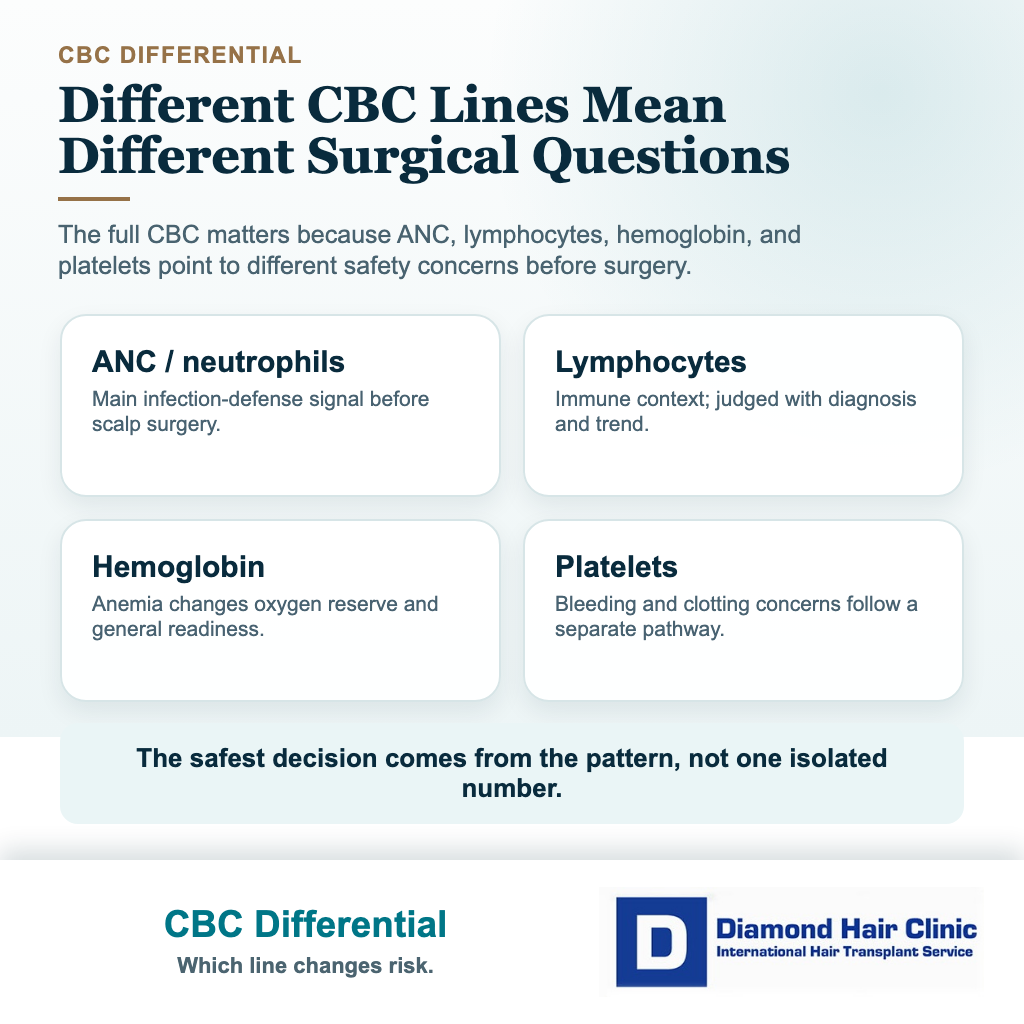
Low WBC also needs to be separated from low ferritin or anemia before a hair transplant. Anemia affects oxygen delivery, stamina, bleeding tolerance, and sometimes the diagnosis behind hair shedding. Low neutrophils mainly raise concern about infection defense. Both can delay surgery, but they do not mean the same thing.
If the count is only mildly low and stable, I may ask for a repeat CBC close to surgery, a note from the treating doctor, or a short delay until the cause is clear. That may feel frustrating, but it is much better than discovering a preventable medical concern on the operating day.
Low results that need repeat testing or hematology review
A repeat test is reasonable when the abnormal result is new, when you recently had a viral illness, when the sample may have been taken during stress or recovery, or when the count does not fit your usual history. Counts can change. A fresh CBC can show whether the result was temporary or still present.
A repeat CBC is most useful when the timing is clear. Tell the clinic if the first test was taken during COVID, flu, dental infection, urinary infection, skin infection, antibiotic treatment, steroid change, or immediately after a difficult travel or illness period. Also say whether symptoms had fully settled before the repeat blood draw.
A hematology or internal medicine review becomes more relevant when neutrophils are clearly low, the result repeats, several blood cell lines are abnormal, there is fever or recurrent infection, unexplained weight loss, easy bruising, mouth ulcers, severe fatigue, or medication known to affect blood counts. Surgery should wait when the medical explanation is still unknown.
Fever with a low neutrophil count is not something to watch casually from home before a cosmetic procedure. The same is true for chills, a new cough, shortness of breath, painful urination, draining wounds, or mouth sores. Those symptoms need medical review before a hair transplant date is treated as fixed.
This is especially true if you are already being monitored because of immune disease, inflammatory bowel disease, lupus, psoriasis, kidney disease, HIV, hepatitis, cancer history, or complex medication use. With HIV or hepatitis before a hair transplant, the label alone is not enough. Viral control, liver health, blood results, medication, and infection status must be understood before surgery.
A hair transplant clinic should not tell you to ignore a very low neutrophil count only because the scalp operation is performed under local anesthesia. Local anesthesia does not remove the need for clean healing. If a medical doctor has already advised waiting or seeing a hematologist, the transplant should not be treated as separate from that advice.
Medicines or recent illness can lower white blood cells
Recent viral illness, some bacterial infections, autoimmune disease activity, nutritional problems, bone marrow conditions, and several medicines can affect white blood cells. I need the medication list because a low count may be part of the treatment story, not a random lab finding.
Medicine that affects the immune system needs a more cautious surgical decision. Prednisone before a hair transplant, methotrexate before a hair transplant, and Humira or biologics before a hair transplant each need a different review. If the medicine is protecting a transplanted organ, organ transplant clearance before FUE becomes a separate safety question. Some medicines can change infection risk, wound healing, blood tests, or the timing of elective surgery.
Do not stop a prescribed medicine on your own to make the CBC look better. A flare of the underlying disease can create more surgical risk than the medicine. The safer route is coordinated timing with the doctor who prescribed the treatment. The same discipline applies to medication before a hair transplant in general. I need the truth, not a simplified medication list.
Send medication names with dose, start date, last dose change, and the reason you take them. This is especially important for immune medicines, recent antibiotics or antivirals, chemotherapy or cancer follow up medicines, antithyroid medicines, seizure medicines, and any drug that your doctor monitors with CBC testing. The question is not only whether the number is low. It is why it is low now.
Recent fever, sore throat, flu symptoms, dental infection, skin infection, or antibiotic treatment also matter. If the low count appears during a recent illness, the body may still be recovering. A cold or flu after a hair transplant can change recovery and follow up decisions, so illness timing deserves attention before surgery as well.
Details to send before travelling
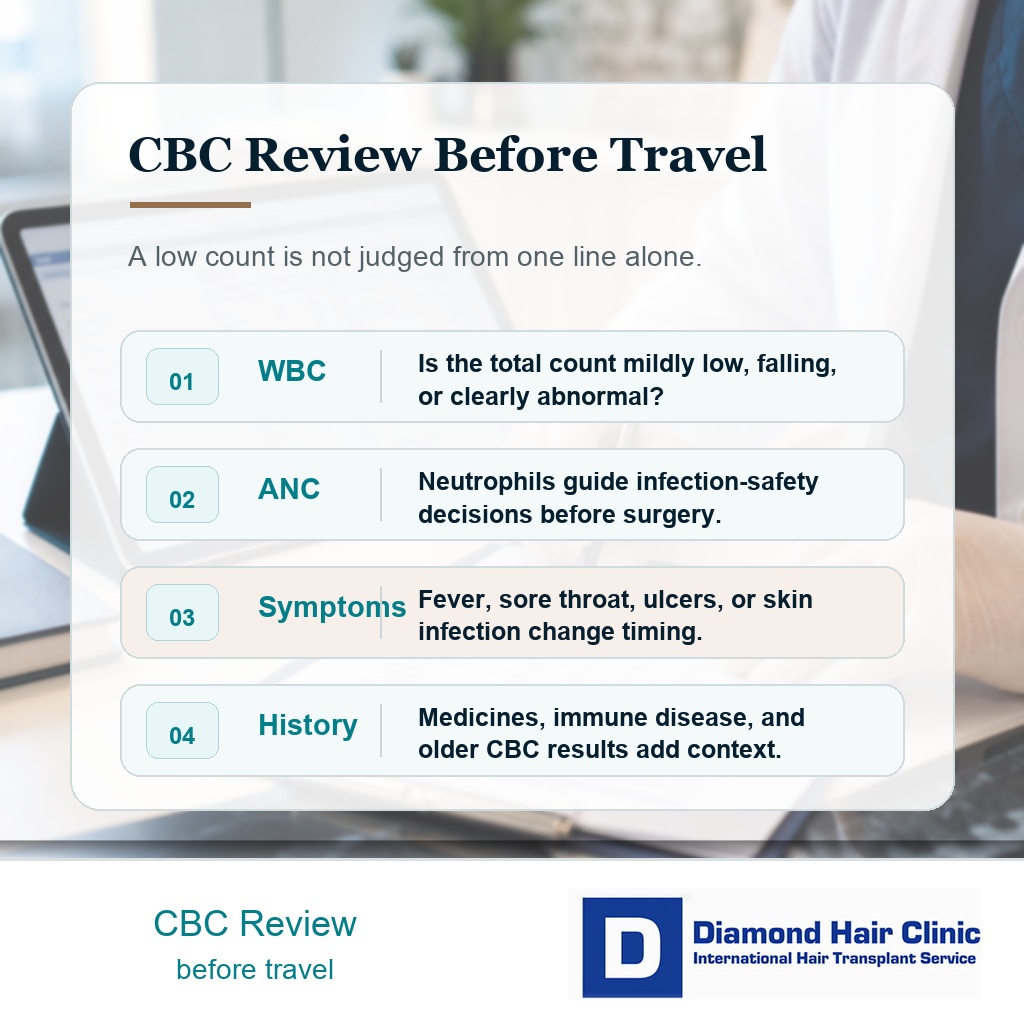
Send the full CBC report, not just the WBC value. I need to see hemoglobin, platelets, total WBC, neutrophils, lymphocytes, and the reference ranges used by that laboratory. If the report has flags or comments, include those as well.
Include the exact WBC, ANC or absolute neutrophil value, lymphocyte value, units, test date, and reference ranges. International reports may use x 109/L, cells per microliter, or different labels for the same cell line. A cropped screenshot of one low WBC number is not enough to decide travel or surgery.
Send the date of the test, any older CBC results for comparison, your medication list, recent infections, chronic diagnoses, and any specialist letters. If you already saw a hematologist or internal medicine doctor, send the written assessment. A verbal “my doctor said it is fine” is less useful than a short written clearance that names the result and the reason surgery is acceptable.
A useful clearance note should say the likely cause of the low count, whether fever or active infection is absent, whether elective scalp surgery with many small skin openings and local anesthesia is acceptable, whether a repeat CBC is needed close to surgery, and whether there are any limits on antibiotics or other medicines after surgery.
For international travel, this step should happen before flights are finalized when possible. I may still need to examine you in person, but obvious blood test concerns can often be handled before travel. That protects your time and avoids pressure on the surgical day.
If the clinic requests a repeat CBC, do it close enough to the planned date to be useful. A normal test from many months ago may not answer a current low result. If the repeat test remains low, the surgical date may need to move.
The 10 low WBC review slides below separate total WBC, ANC, symptoms, recent illness, medicine history, full CBC details, repeat testing, doctor note specifics, multiple abnormal blood lines, and the elective timing decision. Swipe sideways, use the arrows one slide at a time, or choose a number below the image.

Low WBC is different from anemia or low ferritin
Low WBC and low neutrophils are mainly about infection defense. Anemia and low ferritin are mainly about oxygen carrying capacity, iron reserve, general health, and sometimes a medical cause of shedding. They can appear together, but they should not be blended into one vague “blood problem.”
This difference matters because the next step may be different. Low ferritin may lead to iron review, diet history, menstrual bleeding history, gastrointestinal review, or treatment before surgery. Low neutrophils may lead to repeat CBC, infection review, medication review, or hematology assessment. Low platelets would raise a different issue around bleeding and clotting.
When several blood values are abnormal together, the threshold to wait becomes lower. Low neutrophils, low hemoglobin, and symptoms of illness are not the same as one mild stable WBC variation in an otherwise well person. Hair transplant surgery should fit the medical state, not the other way around.
If antibiotics are being considered because of infection concern, antibiotics after a hair transplant are not a substitute for proper diagnosis. A low neutrophil count cannot be “covered” casually with antibiotics just to keep the surgical schedule.
Improved results still need context
If the repeat CBC becomes acceptable and the cause was temporary, surgery may become reasonable again. The timing depends on the original severity, the cause, symptoms, scalp condition, and any advice from the treating doctor.
A recovered blood count after a minor viral illness is different from a count that fluctuates because of an immune condition or medication. A stable result gives the surgical team a clearer starting point. An unstable result means the date should remain flexible.
The transplant plan may also change. If you are recovering from illness, a shorter surgical day, a more conservative graft count, better hydration, closer monitoring, or a delayed date may be safer than a maximum session. Bigger is not safer when the medical baseline is borderline. Donor management still matters, but medical readiness comes first.
The same caution sits behind whether someone can die from a hair transplant. Severe events are rare, but they can still happen. Screening, medication review, infection control, and the willingness to postpone are part of responsible surgery.
Diamond Hair Clinic handles the decision
At Diamond Hair Clinic, a low WBC or low neutrophil result is reviewed before the surgical plan is treated as final. The value itself, the differential count, medical history, current medicines, scalp condition, recent infection history, and any specialist advice all matter.
If the result is mild, stable, explained, and medically cleared, surgery may still be possible. If the count is clearly low, recent, unexplained, or connected with symptoms, the date should wait. You should not be pressured to proceed just because travel is inconvenient to change.
With immune disease, the decision connects with autoimmune disease and hair transplant planning. The scalp must be clean and stable, the donor area must be suitable, and the medical treatment should be stable enough for an elective procedure.
When I do not operate, the reason is not fear of one lab number. It is the combination of uncertain immune status, possible infection vulnerability, unclear diagnosis, or a surgical day that may be less safe than it needs to be. Waiting can feel disappointing, but a delayed operation is easier to accept than a preventable complication.
Before arranging travel, make the blood result clear
If your WBC or neutrophils are low before a hair transplant, do not treat the result as a small administrative obstacle. Ask which part of the white blood cell count is low, repeat the test if advised, send the full report to the clinic, and involve the doctor who knows your medical history.
Do not hide recent illness, fever, antibiotics, immune medication, abnormal blood tests, or specialist follow up. A surgeon can only protect you when the medical picture is clear. The aim is not cancellation. The aim is operating on the right day, with the right information, and with a scalp and body that are ready to heal.
If the result is mild, stable, and cleared, surgery may still go ahead. If the result is moderate, severe, unexplained, or linked with symptoms, delaying the date is the more responsible decision. A hair transplant can wait. The point is to avoid bringing a preventable infection risk into an elective procedure.