Oral Minoxidil Timing Around Surgery
Oral minoxidil is a systemic medication, not a hair supplement. Many patients can use it before or after a hair transplant, but for hair loss I treat it as a low dose medical decision, not an unmonitored tablet added out of anxiety. The decision depends on timing, dose, blood pressure, heart history, swelling history, and whether the patient already tolerates it. If oral minoxidil is added while topical products or shampoos are also changing, too many treatments after FUE can make side effects harder to read.
A patient who is already stable on oral minoxidil may be able to continue it or restart it later after surgery. If a patient has not started yet, I usually avoid beginning during the final 4 weeks before surgery or during the first 10 to 14 days after surgery unless there is a clear medical reason. Starting a new tablet is different from continuing a familiar one.
Stability matters more than adding one more tablet near surgery. I try not to let a patient start a new tablet, stop topical minoxidil, change finasteride, travel, sleep poorly, and have surgery in the same short period. If shedding, swelling, dizziness, or fast heartbeat happens afterward, it becomes much harder to know which factor caused it. For pet owners, the reason for avoiding topical residue belongs in a minoxidil pet safety plan rather than a self directed switch. The same caution applies when hair loss is still moving despite medication before surgery. If oral minoxidil was supplied through an online service, I still want the online hair loss pill proof trail before using the response to adjust graft planning.
The medication may be useful for patients whose case fits, but it should fit into a clear hair loss plan. Oral decisions should sit inside the broader minoxidil after a hair transplant plan. It should not be added out of panic a few days before surgery, and it should not be sold as graft insurance after surgery.
I separate three situations. Continuing a stable prescribed routine, starting oral minoxidil for the first time, and panic use after surgery should not be handled with the same answer. I use the same logic for spironolactone and hair transplant planning. a tolerated stable dose is different from a new or recently changed tablet.
Review blood pressure before deciding on oral minoxidil
The tablet was originally developed as a blood pressure medication. In low doses, many hair loss patients tolerate it well, but the body still sees it as a medication that can affect blood vessels, fluid balance, heart rate, dizziness, and swelling.
Before surgery, the medical picture needs to be predictable. Local anesthesia, adrenaline, travel stress, anxiety, poor sleep, and the length of the procedure can already influence the body. If the medication adds dizziness, palpitations, or ankle swelling, the plan needs more caution.
This discussion belongs with high blood pressure and hair transplant. It also overlaps with beta blockers before hair transplant surgery when the patient uses more than one medicine that can change pulse or pressure. A hair transplant is elective. The safest surgery day is the one where the medical background is clear and stable.
Continuing oral minoxidil may be possible if it is already well tolerated
Sometimes yes, if it has been reviewed properly. A stable dose for months is different from a tablet started last week. A patient who has taken the same dose for months without dizziness, swelling, palpitations, chest discomfort, or blood pressure instability is different from a patient who still does not know how their body responds.
Tolerance also means the dose has been stable. A tablet that was doubled last week is a new variable, even if the patient has used oral minoxidil before. I avoid surgery, travel, swelling, and a dose change all happening at the same time.
I need a clear picture of the dose, timing, recent dose changes, other medications, heart history, blood pressure pattern, and whether the prescribing doctor is involved. I also check whether the patient had shedding when starting or stopping it before.
Sudden medication changes close to surgery make me slow down unless there is a clear reason. But I also do not ignore a systemic medication just because the patient calls it a hair pill.
Avoid starting oral minoxidil right before surgery
The final 4 weeks before surgery should make the plan clearer, not introduce a new variable. If a new medication causes shedding, dizziness, fluid retention, fast heartbeat, sleep disturbance, or anxiety, it can make the surgical plan harder to judge.
Starting too close to surgery can also confuse the patient emotionally. A small medication shed may be mistaken for worsening baldness. A side effect may be mistaken for surgical anxiety. A blood pressure change may create unnecessary concern on the operation day.
If the patient’s hair loss is active and the medication plan is not yet stable, I may slow down the transplant decision. That broader issue is explained in the article about having a hair transplant too early while hair loss is active.
Restart oral minoxidil only when recovery and medical review allow it
For a patient who used it before surgery and tolerated it well, the restart discussion is often around 10 to 14 days after surgery. By then, the fragile first healing phase has passed, scabs are gone or nearly gone, washing is stable, and there is no unusual swelling, dizziness, or heart symptom.
Some patients are better waiting 3 to 4 weeks, especially if they had strong swelling, blood pressure issues, dizziness, anxiety, or a complicated recovery. There is no single perfect day for every patient.
I also separate restarting from starting. Restarting a familiar dose after the scalp has settled is usually simpler than beginning oral minoxidil for the first time while the patient is swollen, anxious, and checking every shed hair. If everything is changing at once, the recovery story becomes noisy.

Oral minoxidil is different from topical minoxidil
Topical minoxidil touches the scalp. That can irritate the recipient area if it is used before the skin is closed and settled. The tablet does not touch the grafts directly, but it affects the whole body.
So the questions are different. With topical treatment, I worry about scalp irritation, dryness, alcohol base, itching, and contact with healing skin. With oral treatment, I worry less about local irritation and more about blood pressure, swelling, palpitations, dizziness, unwanted hair growth, and interaction with other medical issues.
Topical minoxidil has its own timing. Stopping minoxidil before a hair transplant can differ from oral minoxidil because scalp irritation and systemic effects are not the same question.
Shock loss prevention cannot be guaranteed with medication
It may support native hair in patients whose case fits, but I do not present it as a guarantee against shock loss. Shock loss is influenced by miniaturization, surgical trauma, blood supply, inflammation, and the vulnerability of nearby native hairs.
If a patient has weak native hair, medication may be part of a protective plan, but it cannot erase every risk. Native hair shock loss after a hair transplant is usually a timing and vulnerability issue, not something one tablet can promise to prevent.
It helps to know the difference. Medication can support a plan, but it cannot compensate for poor surgical judgment, excessive grafting, or ignoring unstable native hair.
Temporary shedding can happen after starting oral minoxidil
Some patients notice shedding after starting or changing minoxidil. This can be frightening after a hair transplant because the patient is already watching every hair closely.
The timing matters. Shedding after surgery may be normal transplanted hair shedding, native shock loss, medication related shedding, stress shedding, or ongoing androgenetic hair loss. If several changes happen together, the cause becomes harder to identify.
A short increase in shedding after starting or switching minoxidil does not by itself mean the transplant is failing. It means the timing needs to be interpreted carefully, with photos and the full medication history.
A hair transplant during a minoxidil shed is exactly the kind of timing problem where a stable timeline is safer before making big decisions.
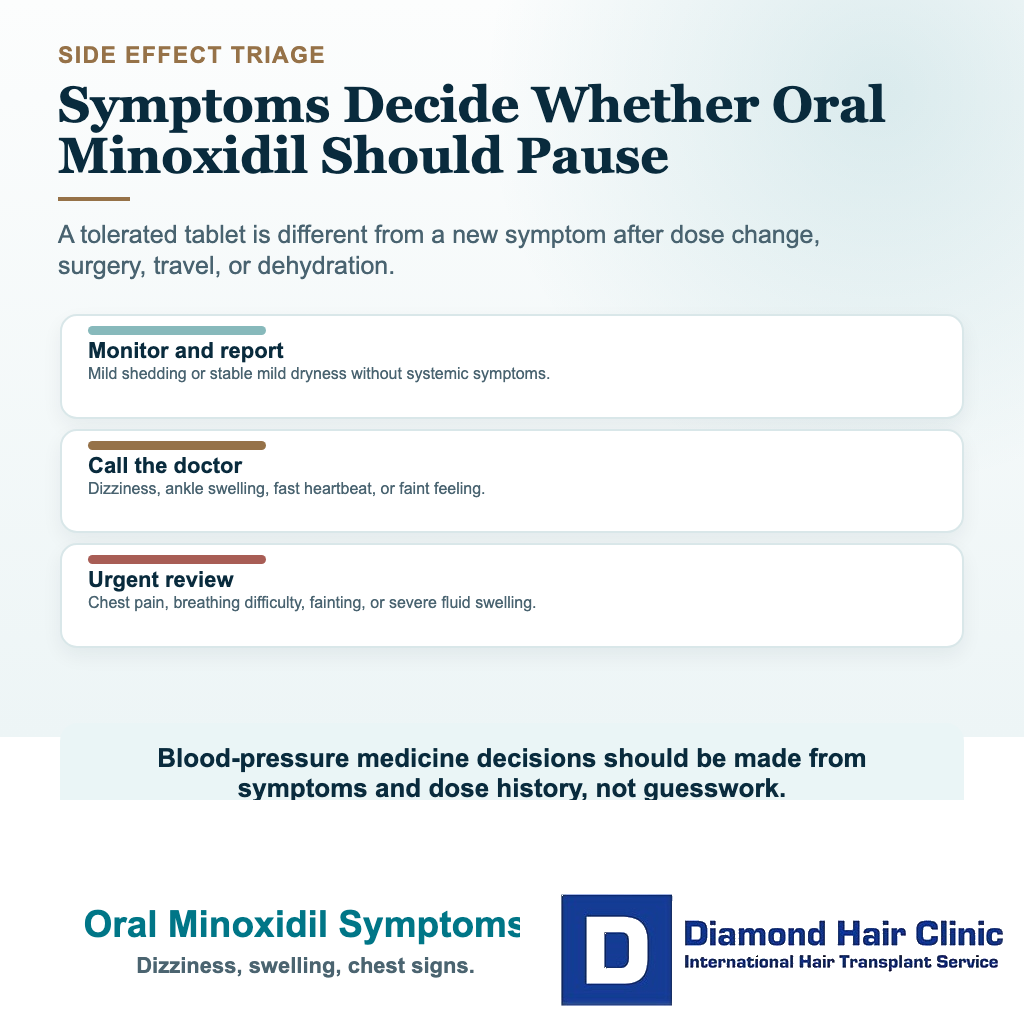
Symptoms that should make a patient contact the doctor
Dizziness, faintness, chest discomfort, fast or irregular heartbeat, shortness of breath, sudden swelling, rapid weight gain, severe headache, or unusual weakness need medical review. These symptoms should not be ignored for the sake of hair.
Unwanted facial or body hair can also occur. That is usually less urgent than heart or swelling symptoms, but it still matters because it affects patient comfort and long term willingness to continue treatment.
If a patient feels unwell on the medication, they should not quietly push through it because they are afraid of losing grafts. Safety comes first, and hair planning can be adjusted after the medical issue is clear.
Some patients need extra caution before taking oral minoxidil
Extra caution is needed for patients who have heart disease or a stent, rhythm problems, low blood pressure, uncontrolled high blood pressure, kidney disease, significant swelling, fainting history, complicated medication use, or unclear blood tests. These patients need medical review before the medication is connected to a transplant plan.
This also applies to patients who combine it with other blood pressure medicines, medicines for erectile dysfunction, stimulants, or aggressive supplement routines. The total medical picture matters because these combinations can change blood pressure, heart rate, dizziness, and swelling.
Full disclosure is not a formality. Medication planning before hair transplant surgery is part of keeping surgery safe.
If oral minoxidil was started because topical products irritated the scalp, I still ask for the full topical history. Online hair loss topicals before FUE can change the way I judge scalp stability and treatment timing.
Use these 8 slides to connect oral minoxidil timing with blood pressure, shedding, and medical review. Swipe across the image, use an arrow, or pick a number below the carousel.